

Treatment Response, Tumor Infiltrating Lymphocytes and Clinical Outcomes in Inflammatory Breast Cancer-Treated with Neoadjuvant Systemic Therapy
- PMID: 38147006
- PMCID: PMC10807408
- DOI: 10.1158/2767-9764.CRC-23-0285
Treatment Response, Tumor Infiltrating Lymphocytes and Clinical Outcomes in Inflammatory Breast Cancer-Treated with Neoadjuvant Systemic Therapy
Abstract
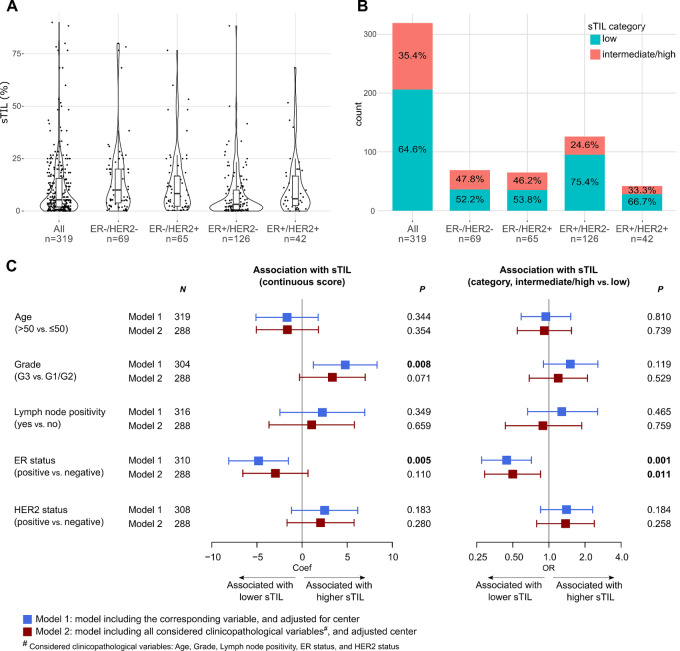
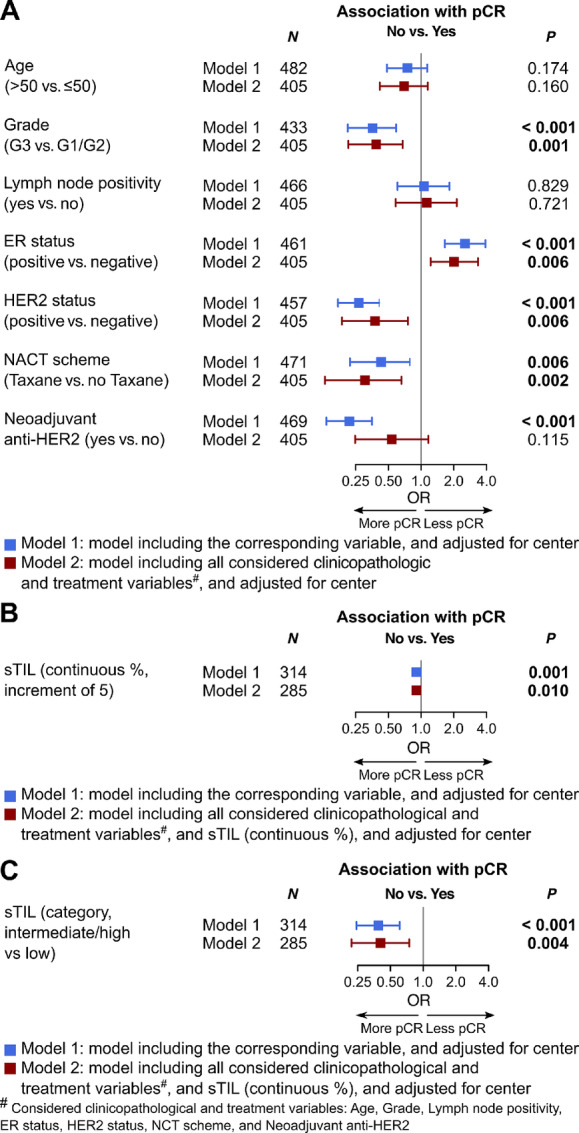
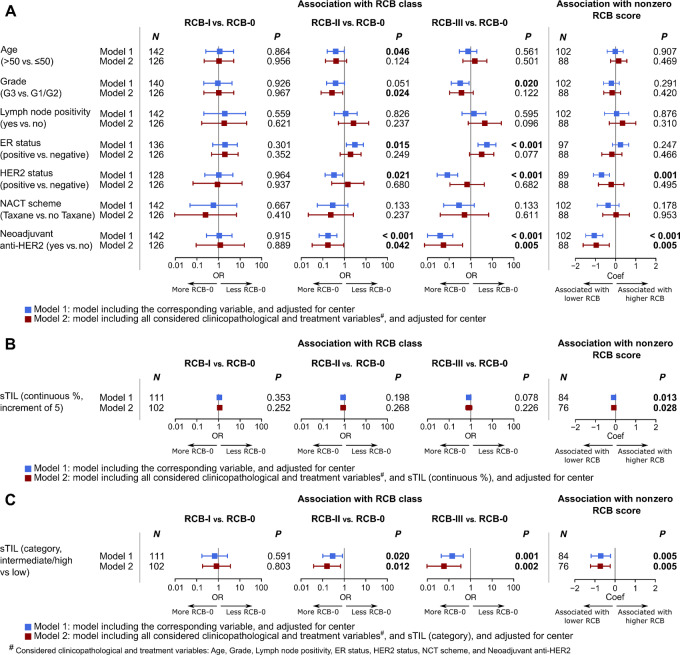
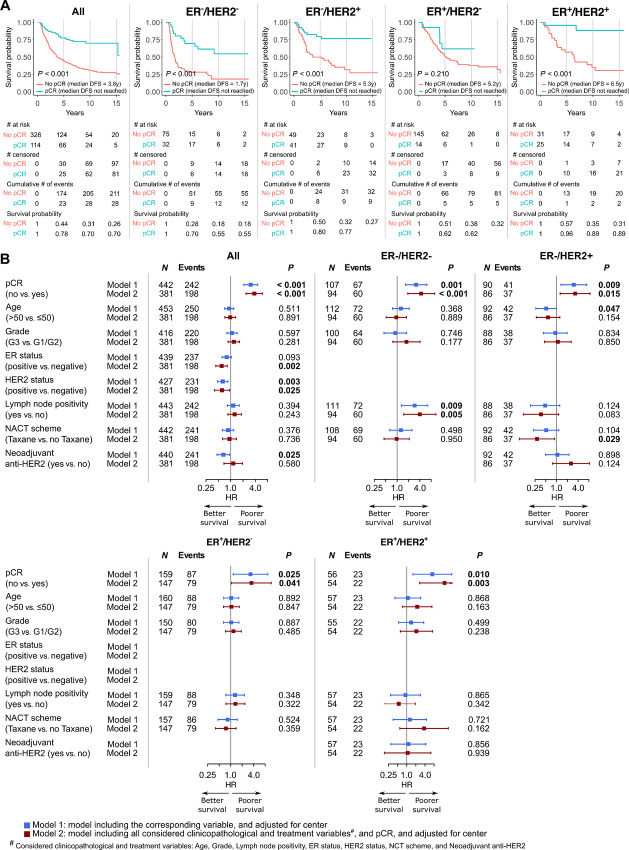
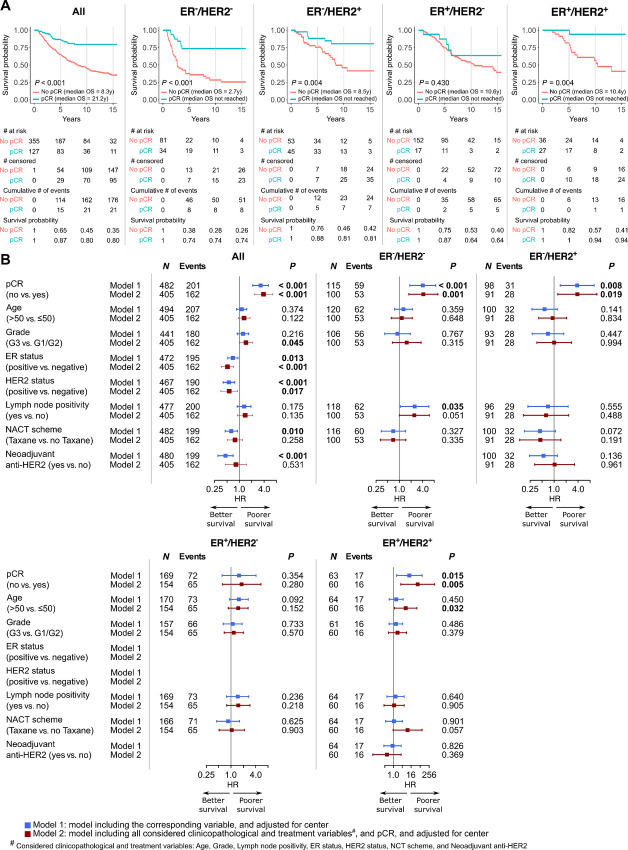
Inflammatory breast cancer (IBC) is a rare (1%-5%), aggressive form of breast cancer, accounting for approximately 10% of breast cancer mortality. In the localized setting, standard of care is neoadjuvant chemotherapy (NACT) ± anti-HER2 therapy, followed by surgery. Here we investigated associations between clinicopathologic variables, stromal tumor-infiltrating lymphocytes (sTIL), and pathologic complete response (pCR), and the prognostic value of pCR. We included 494 localized patients with IBC treated with NACT from October 1996 to October 2021 in eight European hospitals. Standard clinicopathologic variables were collected and central pathologic review was performed, including sTIL. Associations were assessed using Firth logistic regression models. Cox regressions were used to evaluate the role of pCR and residual cancer burden (RCB) on disease-free survival (DFS), distant recurrence-free survival (DRFS), and overall survival (OS). Distribution according to receptor status was as follows: 26.4% estrogen receptor negative (ER-)/HER2-; 22.0% ER-/HER2+; 37.4% ER+/HER2-, and 14.1% ER+/HER2+. Overall pCR rate was 26.3%, being highest in the HER2+ groups (45.9% for ER-/HER2+ and 42.9% for ER+/HER2+). sTILs were low (median: 5.3%), being highest in the ER-/HER2- group (median: 10%). High tumor grade, ER negativity, HER2 positivity, higher sTILs, and taxane-based NACT were significantly associated with pCR. pCR was associated with improved DFS, DRFS, and OS in multivariable analyses. RCB score in patients not achieving pCR was independently associated with survival. In conclusion, sTILs were low in IBC, but were predictive of pCR. Both pCR and RCB have an independent prognostic role in IBC treated with NACT.
Significance: IBC is a rare, but very aggressive type of breast cancer. The prognostic role of pCR after systemic therapy and the predictive value of sTILs for pCR are well established in the general breast cancer population; however, only limited information is available in IBC. We assembled the largest retrospective IBC series so far and demonstrated that sTIL is predictive of pCR. We emphasize that reaching pCR remains of utmost importance in IBC.
© 2024 The Authors; Published by the American Association for Cancer Research.
Figures
References
-
- Abraham HG, Xia Y, Mukherjee B, Merajver SD. Incidence and survival of inflammatory breast cancer between 1973 and 2015 in the SEER database. Breast Cancer Res Treat 2021;185:229–38. - PubMed
-
- Boussen H, Bouzaiene H, ben Hassouna J, Gamoudi A, Benna F, Rahal K. Inflammatory breast cancer in tunisia: reassessment of incidence and clinicopathological features. Semin Oncol 2008;35:17–24. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
