

Balloon pulmonary valvuloplasty: A systematic review
- PMID: 38147974
- PMCID: PMC11143516
- DOI: 10.1016/j.ihj.2023.12.007
Balloon pulmonary valvuloplasty: A systematic review
Abstract
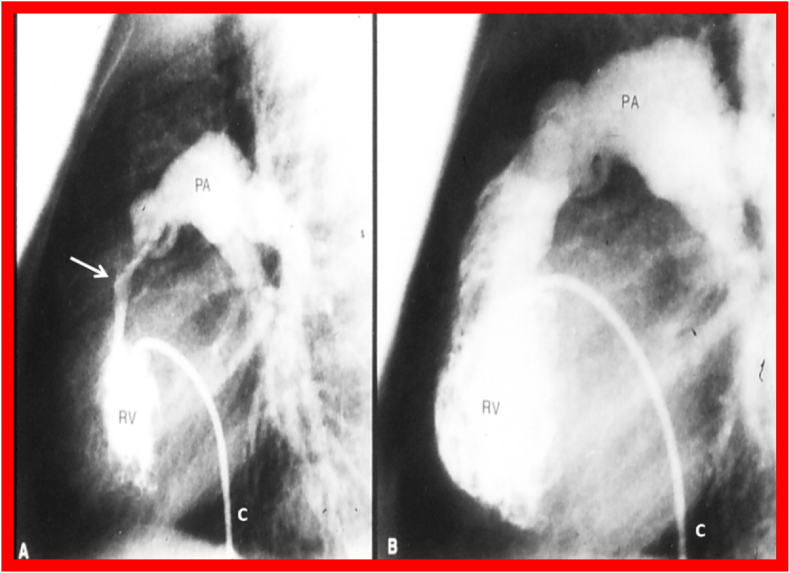
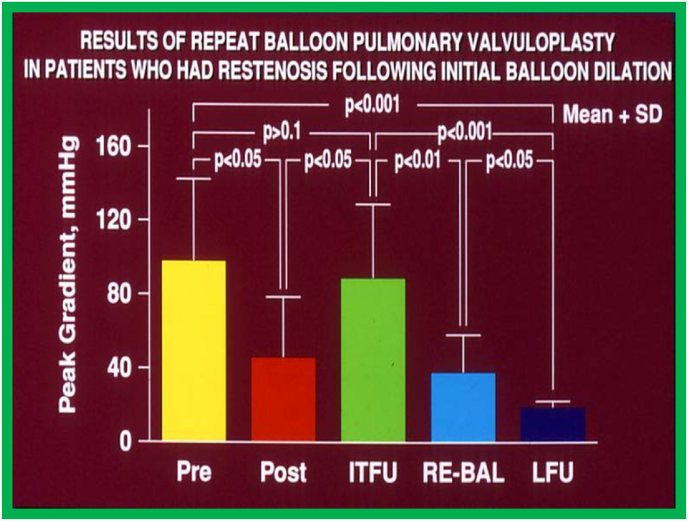
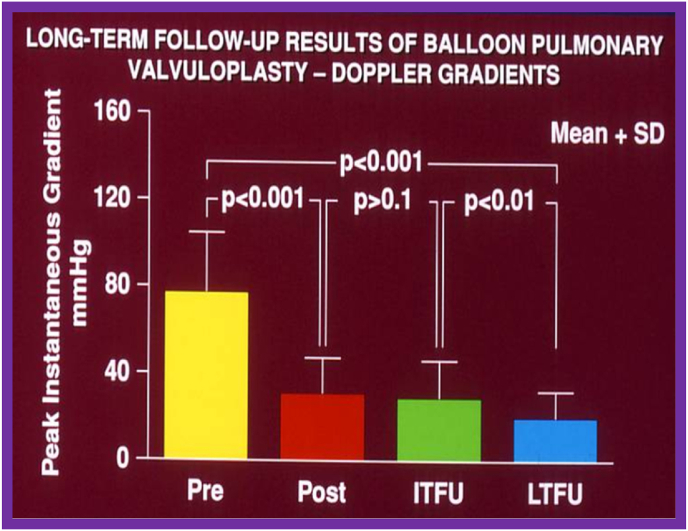
There is conclusive evidence for relief of pulmonary valve obstruction immediately after balloon pulmonary valvuloplasty (BPV) and at follow-up. Development of infundibular obstruction is seen in more severe PS cases and in older subjects. Reappearance of PS was observed in approximately 10 % of patients following BPV. The reasons for recurrence were found to be balloon/annulus ratio less than 1.2 and immediate post-BPV pulmonary valve peak gradients greater than 30 mmHg. Recurrent stenosis is successfully addressed by repeating BPV with lager balloons than used initially. Long-term results revealed continue relief of obstruction, but with development of pulmonary insufficiency, some patients requiring replacement of the pulmonary valve. It was concluded that BPV is the treatment of choice in the management valvar PS and that balloon/annuls ratio used for BPV should be lowered to 1.2 to 1.25. It was also suggested that strategies should be developed to prevent/reduce pulmonary insufficiency at long-term follow-up.
Keywords: Balloon pulmonary valvuloplasty; Long-term results; Pulmonary insufficiency; Pulmonary stenosis; Restenosis.
Copyright © 2023 Cardiological Society of India. Published by Elsevier, a division of RELX India, Pvt. Ltd. All rights reserved.
Conflict of interest statement
Declaration of competing interest 1. The author states that there are no financial or non-financial assistances provided by a third party for the reported work. 2. The author declares that there are no financial interest or relationship related to the subject matter in this manuscript, including advisory positions, consulting fees, equity & stock ownership, and non-financial support. 3. He author declares that there are no patent or copyright issues relevant to the work in the manuscript. 4. There are no other items or issues to merit disclosure.
Figures



References
-
- Grüntzig A., Schneider H.J. [The percutaneous dilatation of chronic coronary stenoses--experiments and morphology] Schweiz Med Wochenschr. 1977;107(44):1588. [Article in German. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
