

An In Silico Platform to Predict Cardiotoxicity Risk of Anti-tumor Drug Combination with hiPSC-CMs Based In Vitro Study
- PMID: 38148384
- PMCID: PMC10879352
- DOI: 10.1007/s11095-023-03644-4
An In Silico Platform to Predict Cardiotoxicity Risk of Anti-tumor Drug Combination with hiPSC-CMs Based In Vitro Study
Abstract
Objective: Antineoplastic agent-induced systolic dysfunction is a major reason for interruption of anticancer treatment. Although targeted anticancer agents infrequently cause systolic dysfunction, their combinations with chemotherapies remarkably increase the incidence. Human induced pluripotent stem cell-derived cardiomyocytes (hiPSC-CMs) provide a potent in vitro model to assess cardiovascular safety. However, quantitatively predicting the reduction of ejection fraction based on hiPSC-CMs is challenging due to the absence of the body's regulatory response to cardiomyocyte injury.
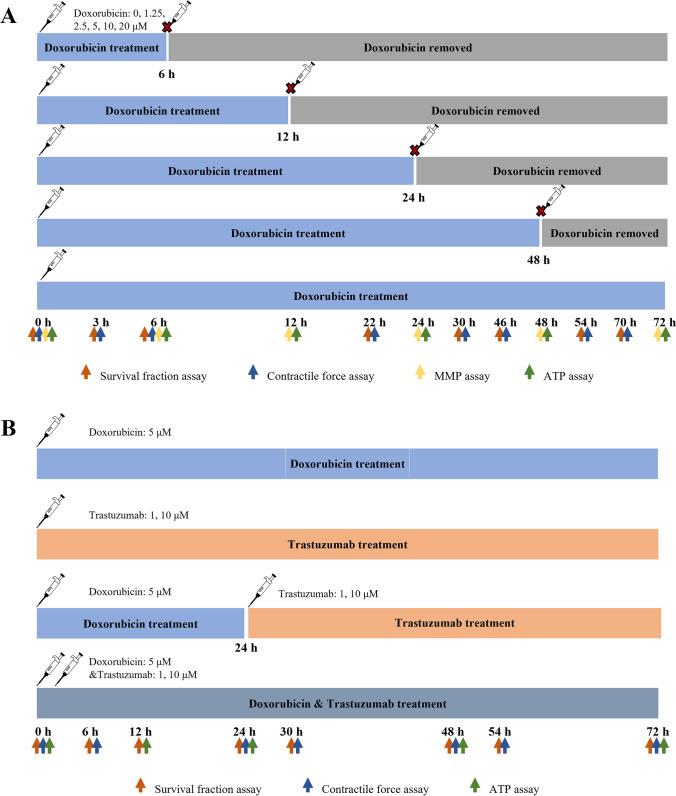
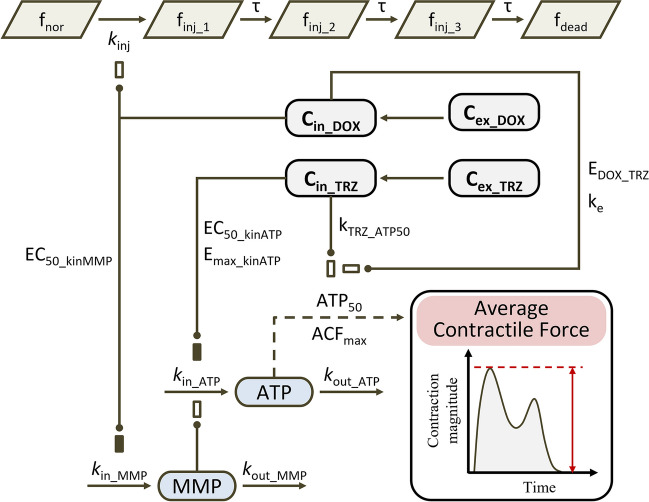
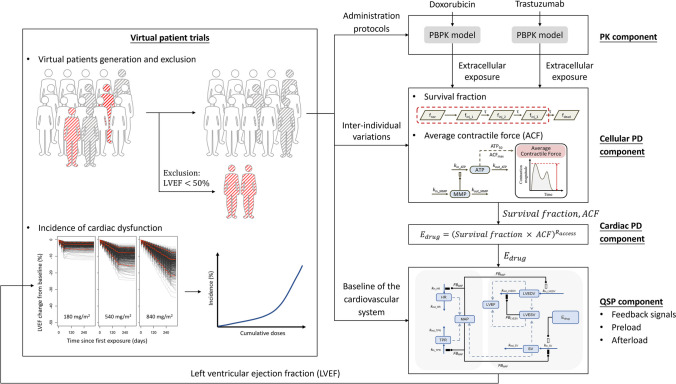
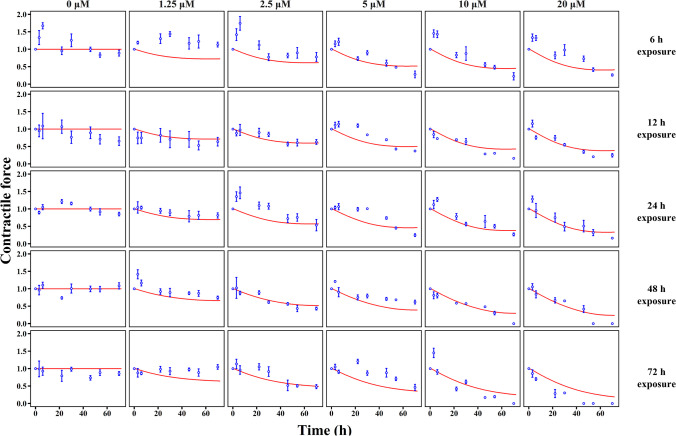
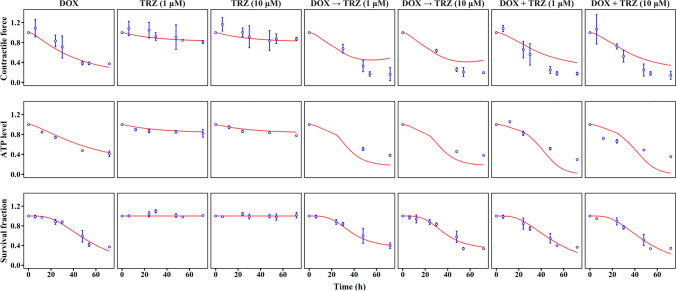
Methods: Here, we developed and validated an in vitro-in vivo translational platform to assess the reduction of ejection fraction induced by antineoplastic drugs based on hiPSC-CMs. The translational platform integrates drug exposure, drug-cardiomyocyte interaction, and systemic response. The drug-cardiomyocyte interaction was implemented as a mechanism-based toxicodynamic (TD) model, which was then integrated into a quantitative system pharmacology-physiological-based pharmacokinetics (QSP-PBPK) model to form a complete translational platform. The platform was validated by comparing the model-predicted and clinically observed incidence of doxorubicin and trastuzumab-induced systolic dysfunction.
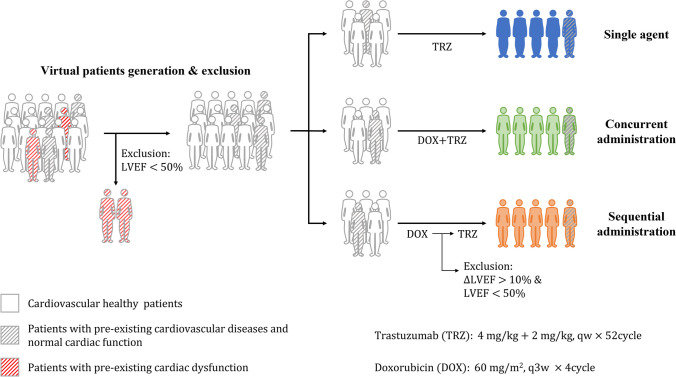
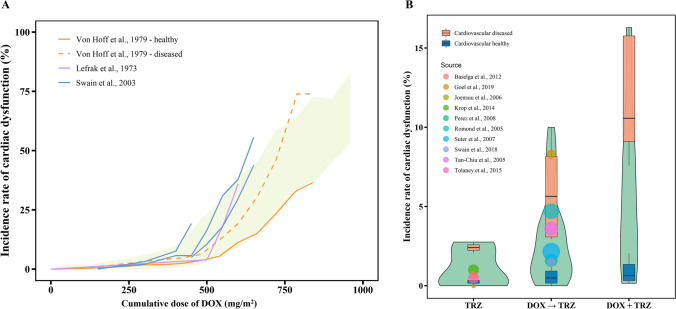
Results: A total of 33,418 virtual patients were incorporated to receive doxorubicin and trastuzumab alone or in combination. For doxorubicin, the QSP-PBPK-TD model successfully captured the overall trend of systolic dysfunction incidences against the cumulative doses. For trastuzumab, the predicted incidence interval was 0.31-2.7% for single-agent treatment and 0.15-10% for trastuzumab-doxorubicin sequential treatment, covering the observations in clinical reports (0.50-1.0% and 1.5-8.3%, respectively).
Conclusions: In conclusion, the in vitro-in vivo translational platform is capable of predicting systolic dysfunction incidence almost merely depend on hiPSC-CMs, which could facilitate optimizing the treatment protocol of antineoplastic agents.
Keywords: cancer therapy; cardiac toxicity; in vitro to in vivo translation; pluripotent stem cells; quantitative systems pharmacology.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
References
-
- Krop IE, Kim SB, Gonzalez-Martin A, LoRusso PM, Ferrero JM, Smitt M, et al. Trastuzumab emtansine versus treatment of physician’s choice for pretreated HER2-positive advanced breast cancer (TH3RESA): a randomised, open-label, phase 3 trial. Lancet Oncol. 2014;15(7):689–99. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
