

Pregnancy outcomes after implementation of an induction of labor care pathway
- PMID: 38148833
- PMCID: PMC10750180
- DOI: 10.1016/j.xagr.2023.100292
Pregnancy outcomes after implementation of an induction of labor care pathway
Abstract
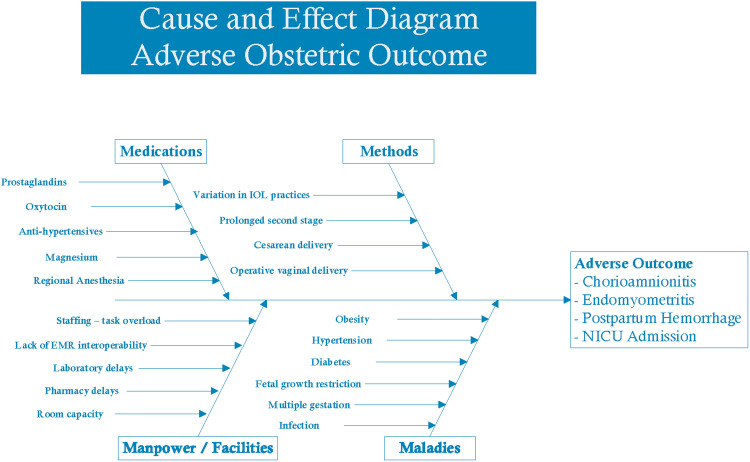
Background: Induction of labor is common; however, the optimum clinical strategy for induction of labor is less clear. Variations in clinical practices related to induction of labor may lead to increased complications and longer induction of labor times.
Objective: This study aimed to analyze whether the implementation of an evidence-based standardized care pathway improves the clinical outcomes associated with induction of labor.
Study design: This was an approved quality improvement project implementing a clinical care pathway for induction of labor. Moreover, this was a retrospective cohort study of inductions of labor for 5 months before (January 2018 to May 2018) and 14 months after (August 2018 to September 2019) the implementation of the care pathway. The primary outcome was time from admission to delivery. Time from admission to delivery was stratified by mode of delivery. The secondary outcomes included chorioamnionitis, endometritis, neonatal intensive care unit admissions, cesarean delivery, postpartum hemorrhage, and a composite of unanticipated outcomes (chorioamnionitis, endometritis, neonatal intensive care unit admissions, cesarean delivery, and postpartum hemorrhage). In addition, pathway adherence was analyzed. The outcomes were analyzed using 2-tailed t tests for continuous data and the Fisher exact test and chi-square tests for categorical data. Propensity score matching was used to assess for confounding by potential covariates.
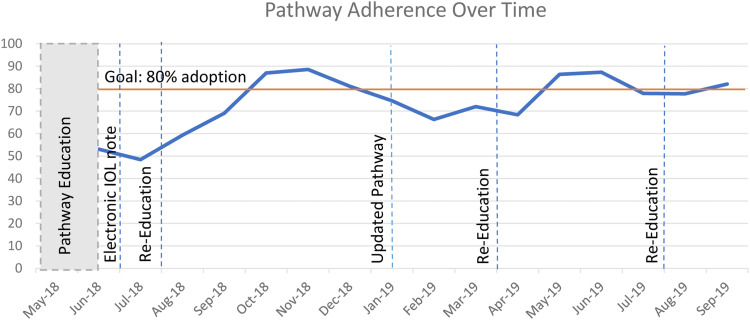
Results: A total of 1471 inductions of labor were reviewed, with 392 inductions of labor before the implementation of the care pathway and 1079 inductions of labor after the implementation of the care pathway. The pathway was associated with a nonsignificant reduction in the time from admission to delivery by 1.2 hours (from 23.4 to 22.2 hours; P=.08). There was a nonsignificant increase in the time to cesarean delivery before (28.2 hours) and after (28.8 hours) protocol implementation (P=.71). There was a significant decrease in the time to delivery by 1.7 hours for vaginal deliveries (from 22.2 to 20.5 hours) after protocol implementation (P=.02). There was a significant decrease in chorioamnionitis (from 12.5% to 6.0%; odds ratio, 0.44; 95% confidence interval, 0.29-0.67), a significant decrease in endometritis (from 6.9% to 2.6%; odds ratio, 0.36; 95% confidence interval, 0.20-0.65), and a significant decrease in composite unanticipated outcomes (from 56.9% to 36.6%; odds ratio, 0.46; 95% confidence interval, 0.34-0.56) after the implementation of the care pathway. There was no significant difference in postpartum hemorrhage (from 7.9% to 6.1%; odds ratio, 0.76; 95% confidence interval, 0.48-1.22), neonatal intensive care unit admissions (from 18.1% to 14.0%; odds ratio, 0.74; 95% confidence interval, 0.54-1.02), or cesarean deliveries (from 19.6% to 20.1%; odds ratio, 1.03; 95% confidence interval, 0.76-1.40) after the implementation of the care pathway. Pathway adherence varied, ranging from 50% to 89%.
Conclusion: The introduction of a standardized induction of labor pathway was associated with a nonsignificant reduction in the time from admission to delivery by 1.2 hours and improved pregnancy outcomes, including decreased infections and unanticipated outcomes. Further opportunities for improvements in clinical outcomes may be realized with increased compliance with the care pathway.
Keywords: clinical care pathway; clinical outcomes; clinical standardization; induction of labor; process improvement.
Figures
References
-
- Simpson KR. Trends in labor induction in the United States, 1989 to 2020. MCN Am J Matern Child Nurs. 2022;47:235. - PubMed
-
- Gestational hypertension and preeclampsia: ACOG practice bulletin, number 222. Obstet Gynecol. 2020;135:e237–e260. - PubMed
-
- American College of Obstetricians and Gynecologists' Committee on Practice Bulletins—Obstetrics ACOG Practice Bulletin No. 203: chronic hypertension in pregnancy. Obstet Gynecol. 2019;133:e26–e50. - PubMed
LinkOut - more resources
Full Text Sources
