

Primary perioperative haemodynamic effects of ß-receptor blockade in patients with catecholamine-secreting tumours
- PMID: 38148968
- PMCID: PMC10749879
- DOI: 10.1016/j.bjao.2023.100240
Primary perioperative haemodynamic effects of ß-receptor blockade in patients with catecholamine-secreting tumours
Abstract
Introduction: Guidelines for the treatment of catecholamine-producing tumours strictly recommend starting ß-receptor blocking medication only after α-receptor blockade has been established. This recommendation is supported only by non-surgical case reports. However, in clinical practice ß-receptor blockade is often started before the diagnosis of a phaeochromocytoma is made. As we routinely treat patients with catecholamine-producing tumours without α-receptor blockade, our aim was to evaluate haemodynamic changes in such patients with and without ß-receptor blockade.
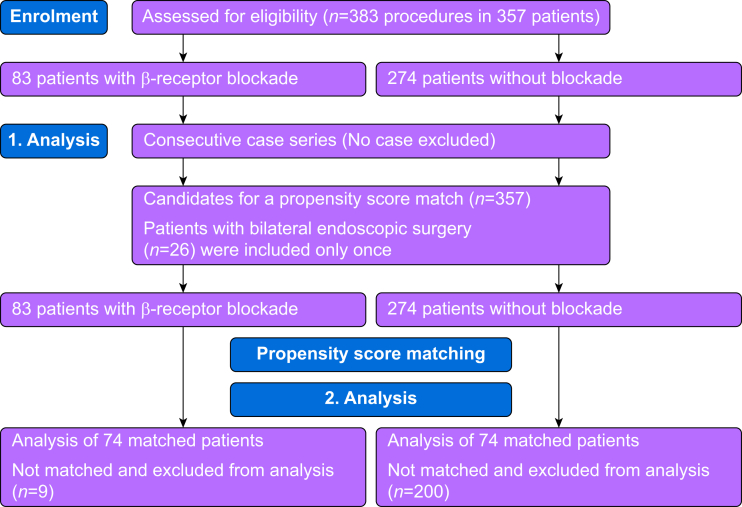
Methods: Perioperative blood pressure was assessed prospectively for all patients. The primary outcome was the highest pre-, intra-, and postoperative systolic blood pressure in patients with or without a ß-receptor blockade. Secondary outcomes were the incidence of intraoperative systolic blood pressure peaks >250 mm Hg and hypotensive episodes. Subsequently, a propensity score matching (PSM) analysis was performed.
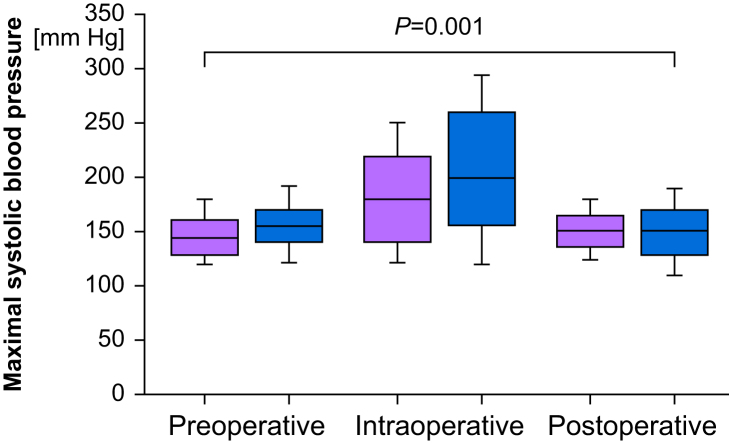
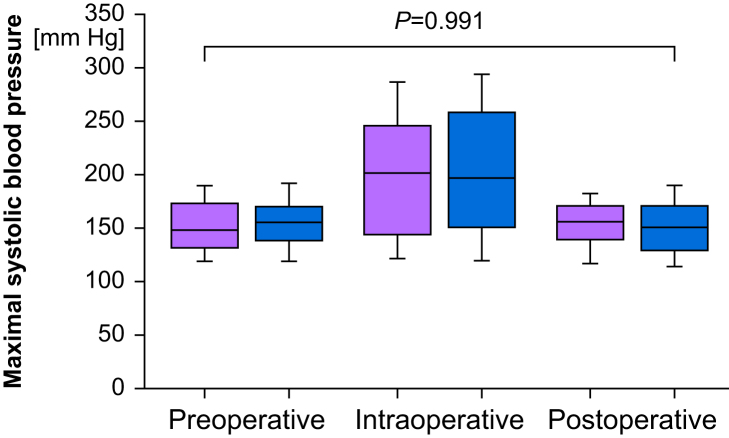
Results: Out of 584 phaeochromocytoma and paraganglioma resections, 383 operations were performed without α-receptor blockade (including 84 with ß-receptor blockade). Before operation and intraoperatively, patients with ß-receptor blockade presented with higher systolic blood pressure (155 [25] and 207 [62] mm Hg) than patients without ß-receptor blockade (147 [24] and 183 [52] mm Hg; P=0.006 and P=0.001, respectively). Intraoperatively, patients with ß-receptor blockade demonstrated a higher incidence of hypotensive episodes (25% without vs 41% with ß-blockade; P<0.001). After propensity score matching no difference between the groups could be confirmed.
Conclusion: Overall, patients with isolated ß-receptor blockade developed higher blood pressure before operation and intraoperatively. After propensity score matching a difference could no longer be detected. Overall, ß-receptor blockade seems to be more a sign for severe disease than a risk factor for haemodynamic instability.
Keywords: adrenal surgery; adrenergic blockade; arterial hypotension; haemodynamic instability; paraganglioma; perioperative management; phaeochromocytoma; risk factors.
© 2023 The Authors.
Figures
References
-
- Lenders J.W.M., Duh Q.Y., Eisenhofer G., et al. Pheochromocytoma and paraganglioma: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2014;99:1915–1942. - PubMed
-
- Hodin R., Lubitz C., Phitayakom R., Stephen A. Diagnosis and management of pheochromocytoma. Curr Probl Surg. 2014;51:151–187. - PubMed
-
- Araujo-Castro M., Pascual-Corrales E., Nattero Chavez L., et al. Protocol for presurgical and anesthetic management of pheochromocytomas and sympathetic paragangliomas: a multidisciplinary approach. J Endocrinol Invest. 2021;44:2545–2555. - PubMed
-
- Kinney M.A.O., Narr B.J., Warner M.A. Perioperative management of pheochromocytoma. J Cardiothorac Vasc Anesth. 2002;16:359–369. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
