

Real-time multi-contrast magnetic particle imaging for the detection of gastrointestinal bleeding
- PMID: 38151569
- PMCID: PMC10752888
- DOI: 10.1038/s41598-023-50041-3
Real-time multi-contrast magnetic particle imaging for the detection of gastrointestinal bleeding
Abstract
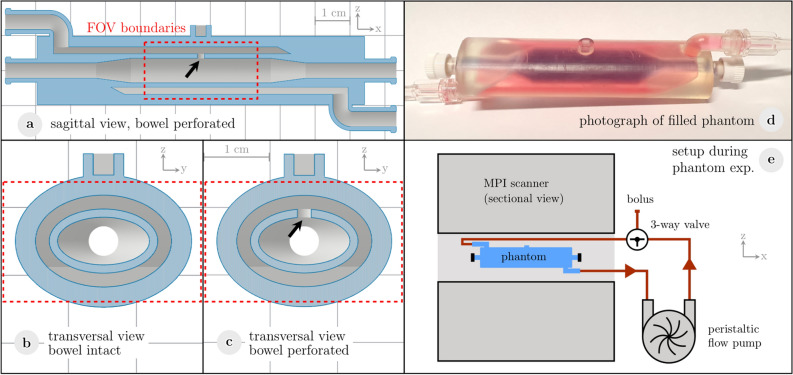
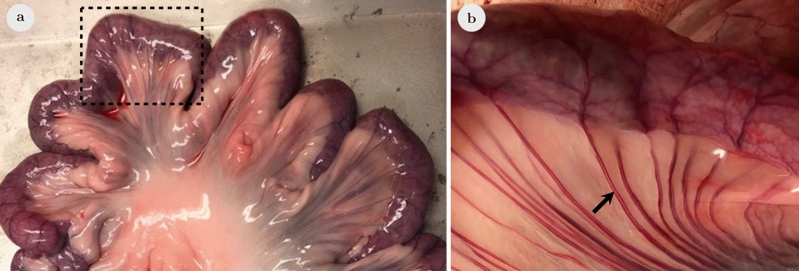
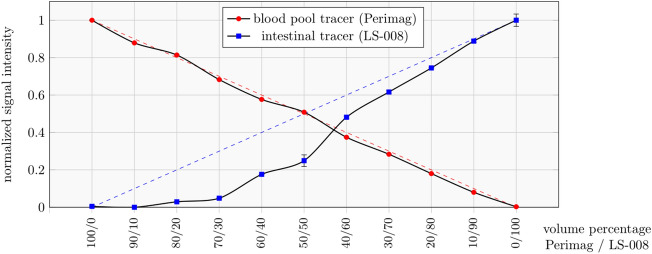
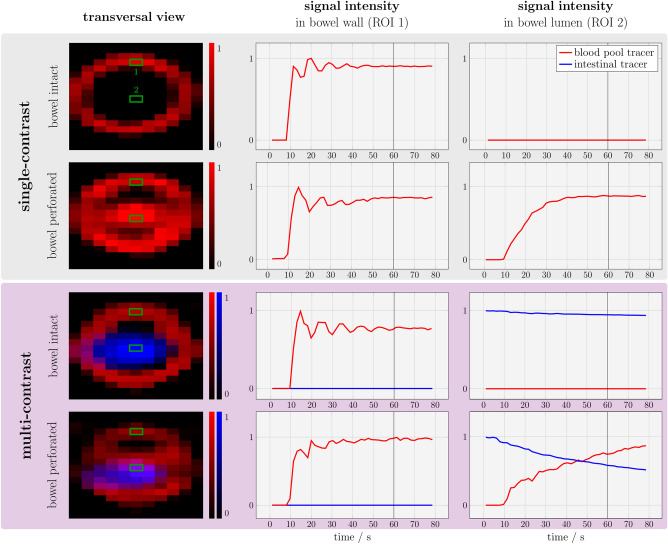
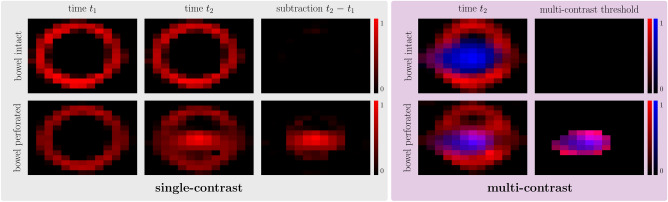
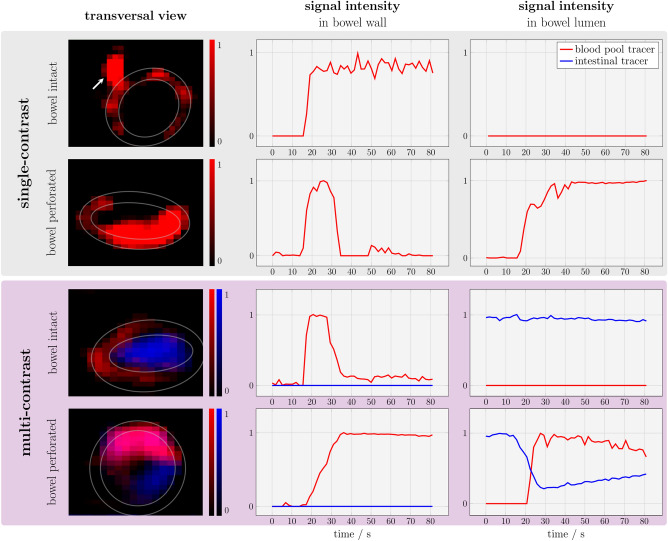
Gastrointestinal bleeding, as a potentially life-threatening condition, is typically diagnosed by radiation-based imaging modalities like computed tomography or more invasively catheter-based angiography. Endoscopy enables examination of the upper gastrointestinal tract and the colon but not of the entire small bowel. Magnetic Particle Imaging (MPI) enables non-invasive, volumetric imaging without ionizing radiation. The aim of this study was to evaluate the feasibility of detecting gastrointestinal bleeding by single- and multi-contrast MPI using human-sized organs. A 3D-printed small bowel phantom and porcine small bowel specimens were prepared with a defect within the bowel wall as the source of a bleeding. For multi-contrast MPI, the bowel lumen was filled with an intestinal tracer representing an orally administered tracer. MPI was performed to evaluate the fluid exchange between the vascular compartment of the bowel wall and the lumen while a blood pool tracer was applied. Leakage of the blood pool tracer was observed to the bowel lumen. Multi-contrast MPI enabled co-registration of both tracers at the same location within the bowel lumen indicating gastrointestinal bleeding. Single- and multi-contrast MPI are feasible to visualize gastrointestinal bleeding. Therefore, MPI might emerge as a useful tool for radiation-free detection of bleeding within the entire gastrointestinal tract.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Advances in Vascular Diagnostics using Magnetic Particle Imaging (MPI) for Blood Circulation Assessment.Adv Healthc Mater. 2024 Sep;13(23):e2400612. doi: 10.1002/adhm.202400612. Epub 2024 Jun 28. Adv Healthc Mater. 2024. PMID: 38879782 Review.
-
Magnetic Particle Imaging for Highly Sensitive, Quantitative, and Safe in Vivo Gut Bleed Detection in a Murine Model.ACS Nano. 2017 Dec 26;11(12):12067-12076. doi: 10.1021/acsnano.7b04844. Epub 2017 Nov 30. ACS Nano. 2017. PMID: 29165995 Free PMC article.
-
Bimodal intravascular volumetric imaging combining OCT and MPI.Med Phys. 2019 Mar;46(3):1371-1383. doi: 10.1002/mp.13388. Epub 2019 Feb 14. Med Phys. 2019. PMID: 30657597
-
In vitro and in vivo comparison of a tailored magnetic particle imaging blood pool tracer with Resovist.Phys Med Biol. 2017 May 7;62(9):3454-3469. doi: 10.1088/1361-6560/aa5780. Epub 2017 Jan 6. Phys Med Biol. 2017. PMID: 28060771
-
Magnetic particle imaging in vascular medicine.Innov Surg Sci. 2018 Oct 9;3(3):179-192. doi: 10.1515/iss-2018-2026. eCollection 2018 Sep. Innov Surg Sci. 2018. PMID: 31579782 Free PMC article. Review.
Cited by
-
Advances in Vascular Diagnostics using Magnetic Particle Imaging (MPI) for Blood Circulation Assessment.Adv Healthc Mater. 2024 Sep;13(23):e2400612. doi: 10.1002/adhm.202400612. Epub 2024 Jun 28. Adv Healthc Mater. 2024. PMID: 38879782 Review.
-
On the partial volume effect in magnetic particle imaging.Phys Med Biol. 2025 Feb 4;70(4):10.1088/1361-6560/ada417. doi: 10.1088/1361-6560/ada417. Phys Med Biol. 2025. PMID: 39902767
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
