

Guideline for the management of myasthenic syndromes
- PMID: 38152089
- PMCID: PMC10752078
- DOI: 10.1177/17562864231213240
Guideline for the management of myasthenic syndromes
Erratum in
-
Erratum to Guideline for the management of Myasthenic Syndromes. Therapeutic Advances in Neurological Disorders. Vol. 16(1): 1-31. DOI 10.1177/17562864231213240.Ther Adv Neurol Disord. 2024 Apr 30;17:17562864241246400. doi: 10.1177/17562864241246400. eCollection 2024. Ther Adv Neurol Disord. 2024. PMID: 38694710 Free PMC article.
Abstract
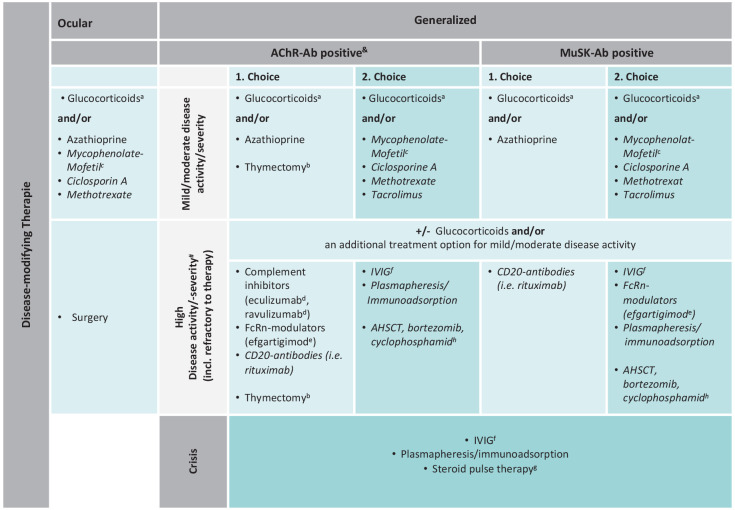
Myasthenia gravis (MG), Lambert-Eaton myasthenic syndrome (LEMS), and congenital myasthenic syndromes (CMS) represent an etiologically heterogeneous group of (very) rare chronic diseases. MG and LEMS have an autoimmune-mediated etiology, while CMS are genetic disorders. A (strain dependent) muscle weakness due to neuromuscular transmission disorder is a common feature. Generalized MG requires increasingly differentiated therapeutic strategies that consider the enormous therapeutic developments of recent years. To include the newest therapy recommendations, a comprehensive update of the available German-language guideline 'Diagnostics and therapy of myasthenic syndromes' has been published by the German Neurological society with the aid of an interdisciplinary expert panel. This paper is an adapted translation of the updated and partly newly developed treatment guideline. It defines the rapid achievement of complete disease control in myasthenic patients as a central treatment goal. The use of standard therapies, as well as modern immunotherapeutics, is subject to a staged regimen that takes into account autoantibody status and disease activity. With the advent of modern, fast-acting immunomodulators, disease activity assessment has become pivotal and requires evaluation of the clinical course, including severity and required therapies. Applying MG-specific scores and classifications such as Myasthenia Gravis Activities of Daily Living, Quantitative Myasthenia Gravis, and Myasthenia Gravis Foundation of America allows differentiation between mild/moderate and (highly) active (including refractory) disease. Therapy decisions must consider age, thymic pathology, antibody status, and disease activity. Glucocorticosteroids and the classical immunosuppressants (primarily azathioprine) are the basic immunotherapeutics to treat mild/moderate to (highly) active generalized MG/young MG and ocular MG. Thymectomy is indicated as a treatment for thymoma-associated MG and generalized MG with acetylcholine receptor antibody (AChR-Ab)-positive status. In (highly) active generalized MG, complement inhibitors (currently eculizumab and ravulizumab) or neonatal Fc receptor modulators (currently efgartigimod) are recommended for AChR-Ab-positive status and rituximab for muscle-specific receptor tyrosine kinase (MuSK)-Ab-positive status. Specific treatment for myasthenic crises requires plasmapheresis, immunoadsorption, or IVIG. Specific aspects of ocular, juvenile, and congenital myasthenia are highlighted. The guideline will be further developed based on new study results for other immunomodulators and biomarkers that aid the accurate measurement of disease activity.
Keywords: Lambert-Eaton myasthenic syndrome; congenital myasthenic syndromes; disease-modifying treatment; myasthenia gravis; myasthenic syndromes; treatment guideline.
© The Author(s), 2023.
Conflict of interest statement
Information on handling authors competing interests, if applicable, is detailed in the German online version of the myasthenia guideline https://register.awmf.org/de/leitlinien/detail/030-087
Figures
References
-
- Wiendl H, Meisel A, Abicht A, et al. Diagnostik und Therapie myasthener Syndrome, S2k-Leitlinie, https://dnvp9c1uo2095.cloudfront.net/cms-content/030087_LL_Myasthenia_gr... (2022, accessed 23 May 2023).
-
- Howard JF, Jr, Utsugisawa K, Benatar M, et al. Safety and efficacy of eculizumab in anti-acetylcholine receptor antibody-positive refractory generalised myasthenia gravis (REGAIN): a phase 3, randomised, double-blind, placebo-controlled, multicentre study. Lancet Neurol 2017; 16: 976–986. - PubMed
-
- Narang P. Ultomiris approved in Europe for the treatment of adults with generalised myasthenia gravis [Press release]. AstraZeneca, https://pharmashots.com/press-releases/ultomiris-approved-in-europe-for-... (2022, accessed 23 September 2022).
Publication types
LinkOut - more resources
Full Text Sources
