

Contemporary surgical techniques for mitral valve replacement in extensive mitral annular calcification
- PMID: 38152201
- PMCID: PMC10750984
- DOI: 10.1016/j.xjtc.2023.10.009
Contemporary surgical techniques for mitral valve replacement in extensive mitral annular calcification
Abstract
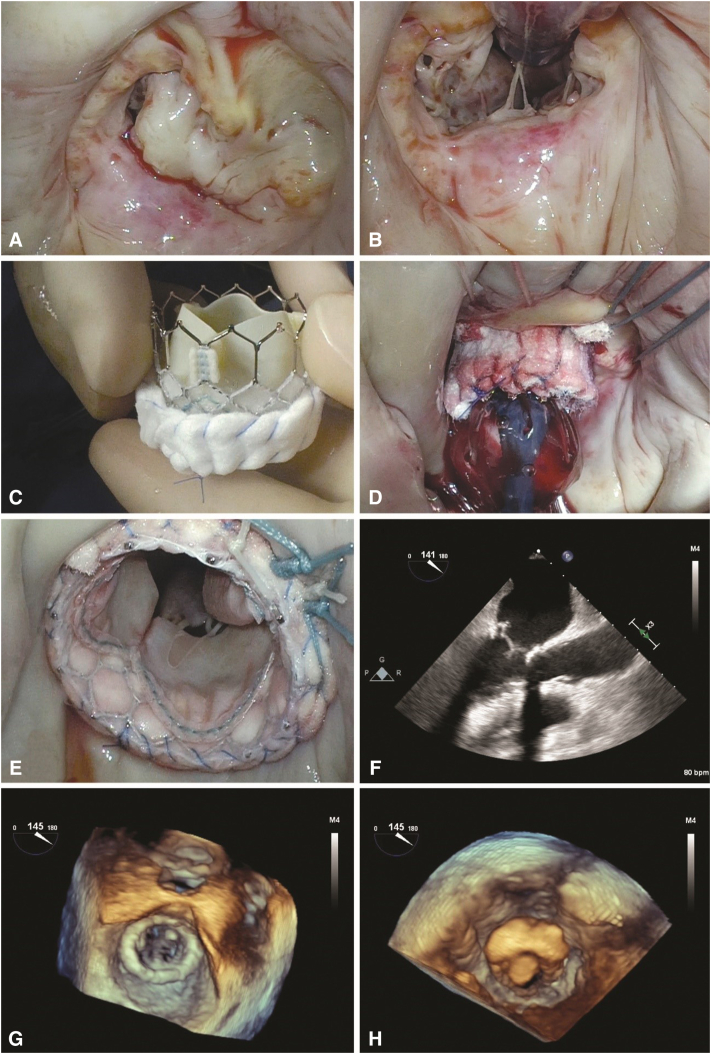
Objectives: Mitral annular calcification remains a formidable lesion in cardiac surgery with significant perioperative morbidity and mortality, particularly when en bloc annular decalcification is implemented. Respect strategies and hybrid approaches have provided safe alternatives. We report the short-term results of our institution's experience with mitral valve replacement in patients with extensive annular calcification.
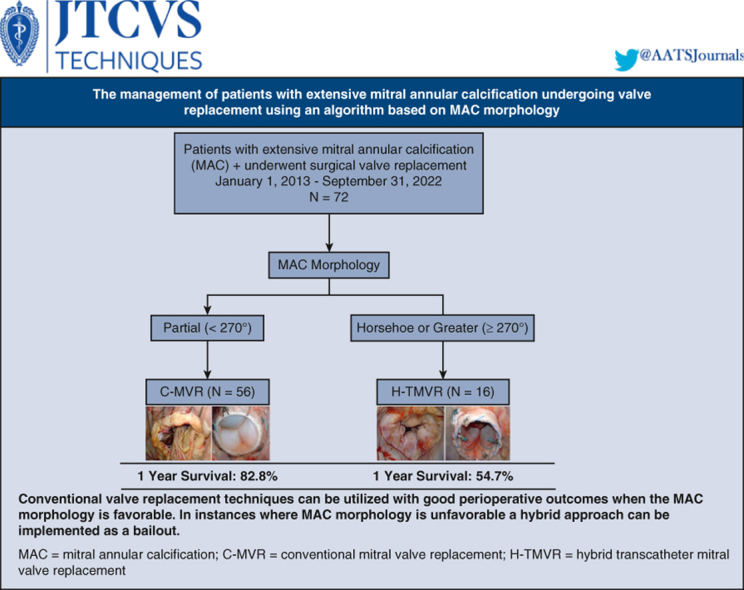
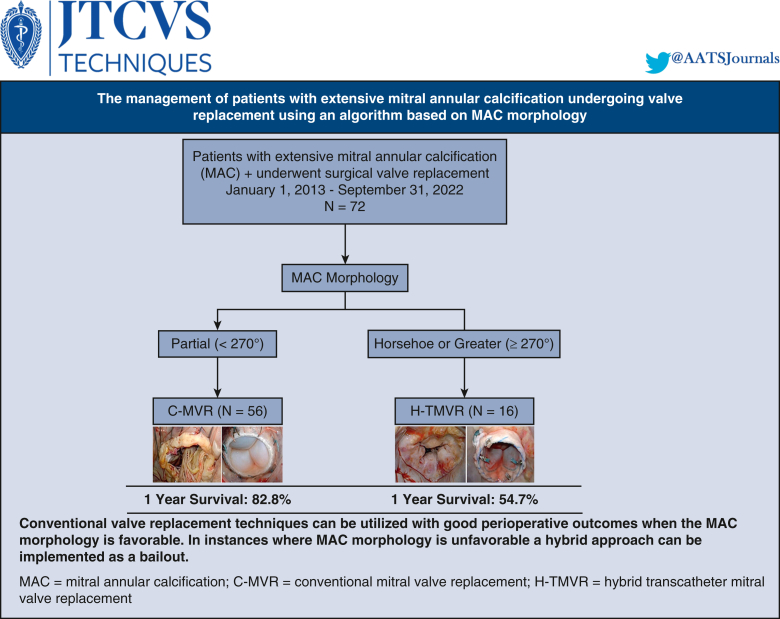
Methods: This is a retrospective review of 72 consecutive patients with extensive annular calcification who underwent open surgical mitral valve replacement from January 1, 2013, to September 31, 2022. Degree of annular calcification was graded as partial, horseshoe, or circumferential. We excluded patients with calcification involving less than one-third of the annulus and patients with rheumatic heart disease.
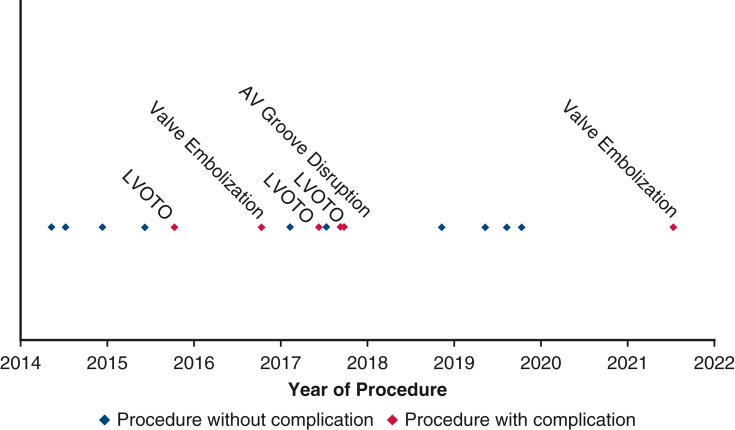
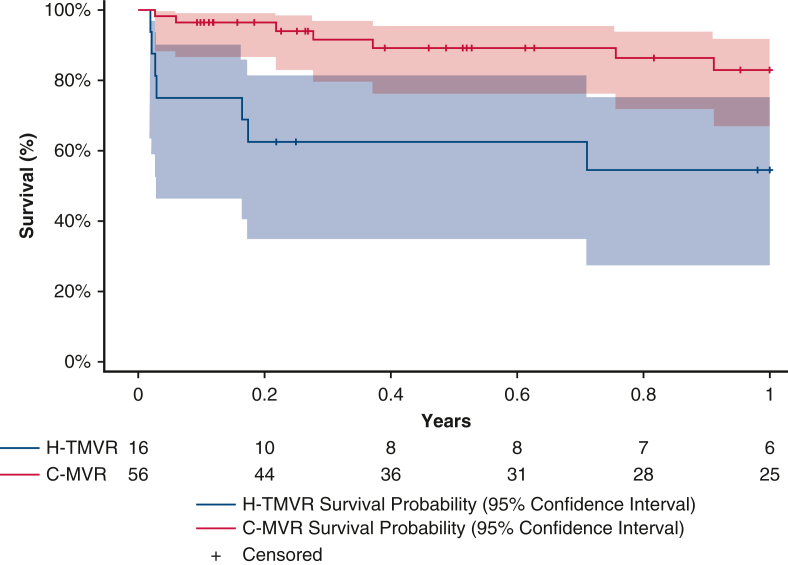
Results: Mean patient age was 71.6 ± 10.9 years, and 50 (69.4%) were female. There were 51 patients (70.8%) with New York Heart Association class 3 or greater and 47 patients (65.3%) with pulmonary hypertension. There were 41 patients (56.9%) with partial, 12 patients (16.7%) with horseshoe, and 19 patients (26.4%) with circumferential calcification. Fifty-six patients (77.8%) underwent conventional valve replacement. Sixteen patients underwent a hybrid procedure using balloon-expandable devices. Concomitant procedures were performed in 61 patients (84.7%). In-hospital mortality and 1-year survival were 3.57% and 82.8% in the standard valve replacement cohort and 25.0% and 54.7% in the hybrid cohort, respectively.
Conclusions: Conventional mitral valve replacement using respect strategies is safe and associated with good outcomes in patients with extensive annular calcification. Hybrid approaches using novel devices should remain as a bailout in select patients because of higher perioperative risks and poor short-term outcomes.
Keywords: annular calcification; hybrid valve replacement; mitral valve.
© 2023 The Author(s).
Conflict of interest statement
D.H.A. is the National Co-Principal Investigator of the TRILUMINATE U.S. Pivotal Trial (Abbott), the ReChord FDA Pivotal Trial (NeoChord), the APOLLO FDA Pivotal Trial (Medtronic), and the CoreValve U.S. Pivotal Trial (Medtronic). The Icahn School of Medicine at Mount Sinai receives royalty payments from Edwards Lifesciences and Medtronic for intellectual property related to Dr Adams' involvement in the development of 2 mitral valve repair rings and 1 tricuspid valve repair ring. G.H.L.T. is a consultant and physician advisory board member for Medtronic and Abbott Structural Heart, a physician advisory board member for Boston Scientific and JenaValve, and a consultant for NeoChord, and has received speaker's honoraria from Siemens Healthineers and East End Medical. All other authors reported no conflicts of interest. The Journal policy requires editors and reviewers to disclose conflicts of interest and to decline handling or reviewing manuscripts for which they may have a conflict of interest. The editors and reviewers of this article have no conflicts of interest.
Figures

References
-
- Fann J.I., Ingels N.B., Jr., Miller D.C. In: Cardiac Surgery in the Adult. 5th ed. Cohn L.H., Adams D.H., editors. McGraw-Hill Education; 2018. Pathophysiology of mitral valve disease.
-
- El-Eshmawi A., Love B., Bhatt H.V., Pawale A., Boateng P., Adams D.H. Direct access implantation of a melody valve in native mitral valve: a hybrid approach in the presence of extensive mitral annular calcification. Ann Thorac Surg. 2015;99:1085. doi: 10.1016/j.athoracsur.2014.10.018. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
