

Total aortic arch replacement without deep hypothermic circulatory arrest in type A aortic dissection: Left axillar artery for arterial cannulation
- PMID: 38152213
- PMCID: PMC10750496
- DOI: 10.1016/j.xjtc.2023.08.020
Total aortic arch replacement without deep hypothermic circulatory arrest in type A aortic dissection: Left axillar artery for arterial cannulation
Abstract
Objective: Total aortic arch replacement (TAR) necessitates hypothermic circulatory arrest (CA). The frozen elephant trunk technique (FET) additionally requires commercial hybrid grafts. Herein we describe a novel modified FET technique without CA using standard grafts thanks to left axillary artery (LAxA) cannulation in patients with acute type A aortic dissection.
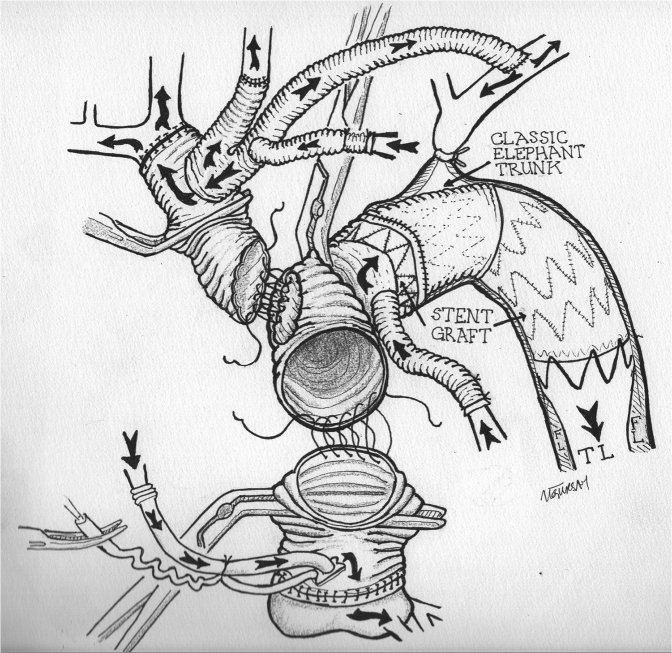
Methods: LAxA anastomosis is made first using a homemade debranching graft, and cardiopulmonary bypass is initiated, followed by anastomoses of left common carotid and innominate arteries. The rest of the operation is performed with complete cerebral perfusion. Following replacement of ascending aorta/root, cardiac reperfusion is started using a root cannula which continues throughout the procedure. Distal arch anastomosis is performed clamp-on, allowing lower body perfusion via left subclavian artery. Lower body perfusion is interrupted for 5 to 8 minutes to deploy an endograft to complete a modified FET. Following cannulation of distal arch graft, perfusion of distal aorta is restarted, and all three grafts are incorporated to construct a neo-ascending aorta and arch.
Results: Between December 2018 and May 2022, 38 patients underwent TAR without operative mortality. Hospital mortality was %15.7, and spinal cord ischemia and stroke were not encountered in surviving patients. The mean lower body CA time was 7.2 ± 2.8 minutes.
Conclusions: TAR using standard endografts without CA is possible with LAxA cannulation. To perform a FET, only a short interruption of lower body circulation is sufficient to deploy an endograft, also improving hemostasis of distal anastomosis. Further studies are required with a higher number of patients to evaluate the efficiency of this novel technique.
Keywords: circulatory arrest; deep hypothermia; frozen elephant trunk; left axillary artery cannulation; total arch replacement; type A aortic dissection.
© 2023 The Author(s).
Conflict of interest statement
The authors reported no conflicts of interest. The Journal policy requires editors and reviewers to disclose conflicts of interest and to decline handling or reviewing manuscripts for which they may have a conflict of interest. The editors and reviewers of this article have no conflicts of interest.
Figures





References
-
- Isselbacher E.M., Preventza O., Black J.H., III, Augoustides J.G., Beck A.W., Bolen M.A., et al. 2022 ACC/AHA Guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on clinical practice guidelines. J Am Coll Cardiol. 2022;80:e223–e393. - PMC - PubMed
-
- Conzelmann L.O., Weigang E., Mehlhorn U., Abugameh A., Hoffmann I., Blettner M., et al. GERAADA Investigators. Mortality in patients with acute aortic dissection type A: analysis of pre-and intraoperative risk factors from the German Registry for Acute Aortic Dissection Type A (GERAADA) Eur J Cardio Thorac Surg. 2016;49:e44–e52. - PubMed
-
- Mousavizadeh M., Daliri M., Aljadayel H.A., Mohammed I., Rezaei Y., Bashir M., et al. Hypothermic circulatory arrest time affects neurological outcomes of frozen elephant trunk for acute type A aortic dissection: a systematic review and meta-analysis. J Card Surg. 2021;36:3337–3351. - PubMed
-
- Shrestha M., Fleissner F., Ius F., Koigeldiyev N., Kaufeld T., Beckmann E., et al. Total aortic arch replacement with frozen elephant trunk in acute type A aortic dissections: are we pushing the limits too far? Eur J Cardio Thorac Surg. 2015;47:361–366. - PubMed
-
- Poon S.S., Tian D.H., Yan T., Harrington D., Nawaytou O., Kuduvalli M., et al. Frozen elephant trunk does not increase incidence of paraplegia in patients with acute type A aortic dissection. J Thorac Cardiovasc Surg. 2020;159:1189–1196. - PubMed
LinkOut - more resources
Full Text Sources
