

The cervical branch-first technique in complex resternotomy
- PMID: 38152225
- PMCID: PMC10750887
- DOI: 10.1016/j.xjtc.2023.08.030
The cervical branch-first technique in complex resternotomy
Abstract
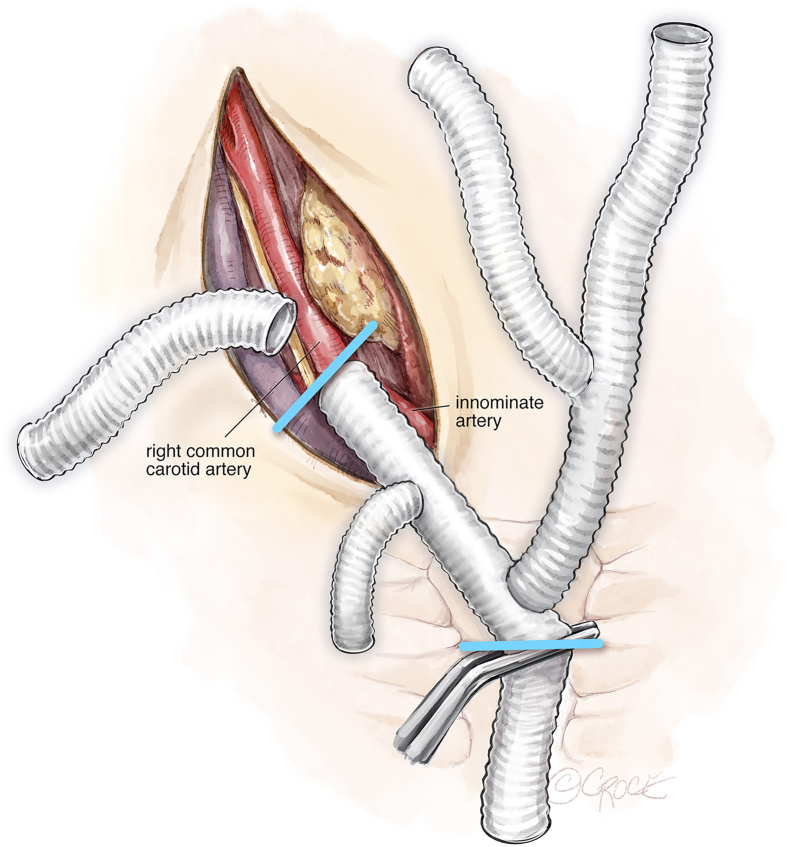
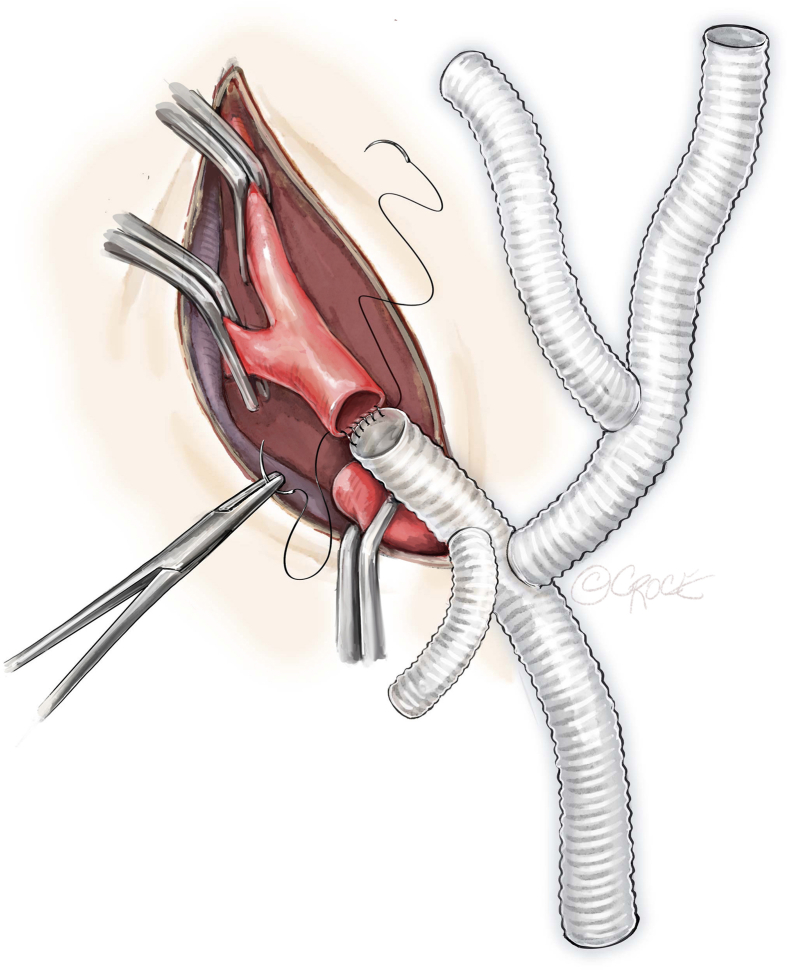
Background: Branch-first total aortic arch repair is a paradigm shift in the technical approach for uninterrupted neuroprotection during open aortic surgery. This technique is further modified to instigate hazardous sternal reentry in patients with hostile mediastinal anatomy at risk of aortic injury.
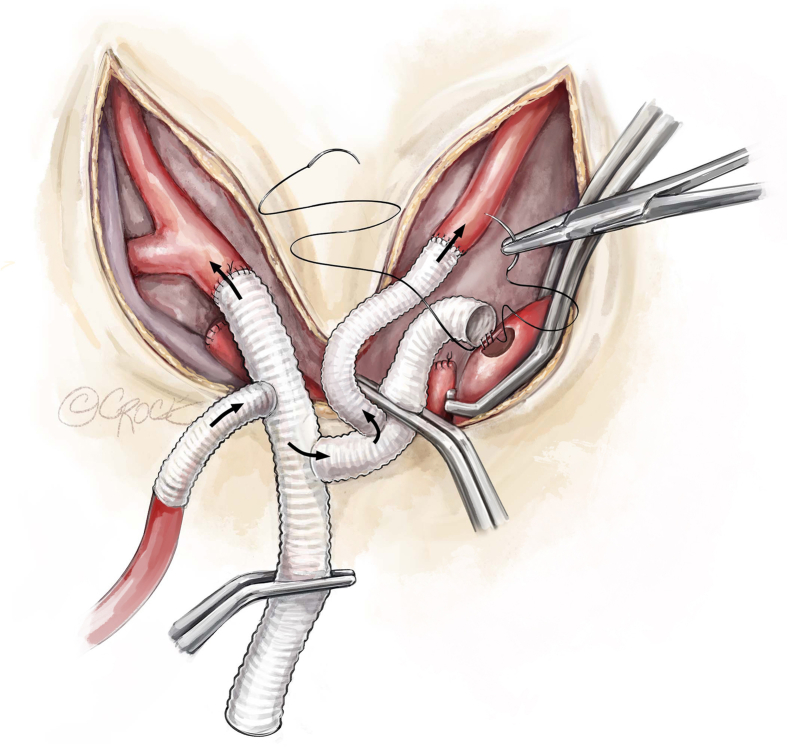
Methods: Intraoperative preparation and the illustrated operative technique of the cervical branch-first technique are described. The accompanying case series narrates the experiences and outcomes of 4 patients who underwent successful complex reoperative aortic surgery utilizing this technique.
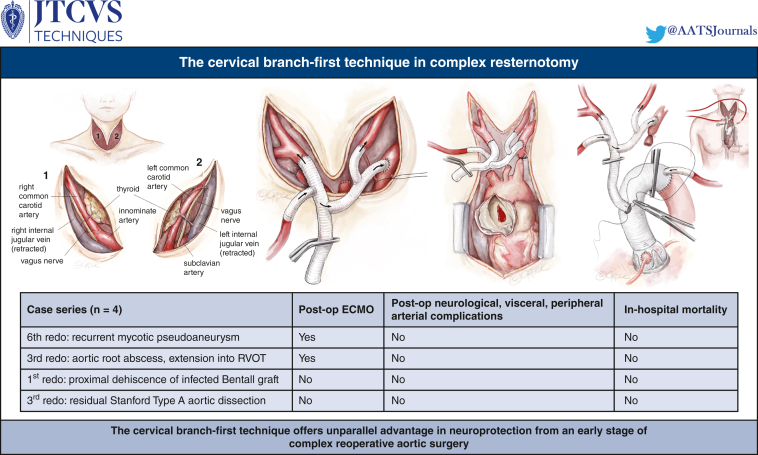
Results: The indications for resternotomy included a sixth reoperation for recurrent mycotic aortic pseudoaneurysm, a third reoperation for extensive infective endocarditis, a reoperation for complete Bentall graft dehiscence with contained aortic rupture, and a third reoperation for residual type A dissection. All patients survived their proposed surgery. Two patients were operated on in an emergency setting. Two patients separated from cardiopulmonary bypass with extracorporeal support. None experienced permanent neurological sequelae, gut ischemia, peripheral arterial complications, or in-hospital mortality. One mortality due to decompensated heart failure was reported at 6 months postoperatively.
Conclusions: The cervical branch-first technique offers unparalleled advantage in neuroprotection from an early stage of complex reoperative aortic surgery. It provides an independent circuit for complete antegrade cerebral perfusion, irrespective of suspension to circulatory flows to the rest of the body during complex reentry into hostile chests. Our experience to date has demonstrated promising outcomes and further refinements will guide patient selection best suited for this technique.
Keywords: branch-first total arch repair; complex redo sternotomy; redo open aortic surgery.
© 2023 The Author(s).
Conflict of interest statement
The authors reported no conflicts of interest. The Journal policy requires editors and reviewers to disclose conflicts of interest and to decline handling manuscripts for which they may have a conflict of interest. The editors and reviewers of this article have no conflicts of interest.
Figures









References
-
- Kim M., Matalanis G. Illustrated technique of “branch-first” total aortic arch replacement. Operative Technique Thorac Cardiovasc Surg. 2020;27:23–38.
-
- McGiffin D. LV vent. https://ecmo.icu/procedures-lv-vent
LinkOut - more resources
Full Text Sources
