

Assessment of effectiveness and safety of thrombolytic therapy to pulmonary emboli by endobronchial ultrasound-guided transbronchial needle injection
- PMID: 38152238
- PMCID: PMC10750838
- DOI: 10.1016/j.xjtc.2023.09.005
Assessment of effectiveness and safety of thrombolytic therapy to pulmonary emboli by endobronchial ultrasound-guided transbronchial needle injection
Abstract
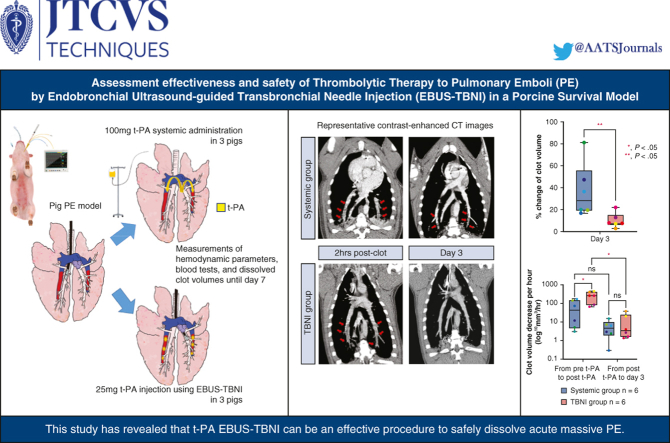
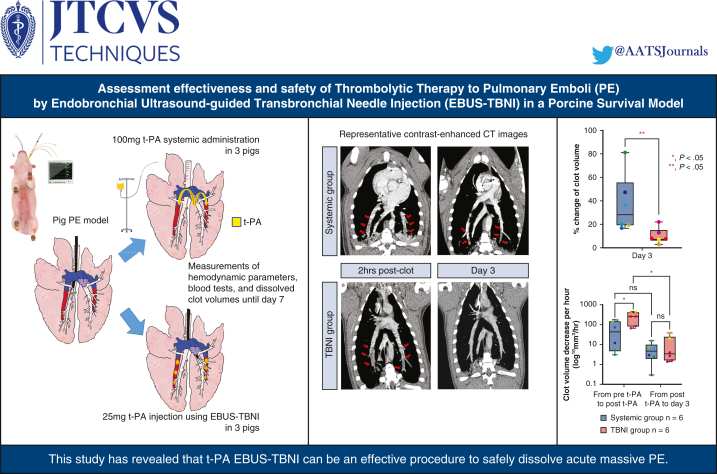
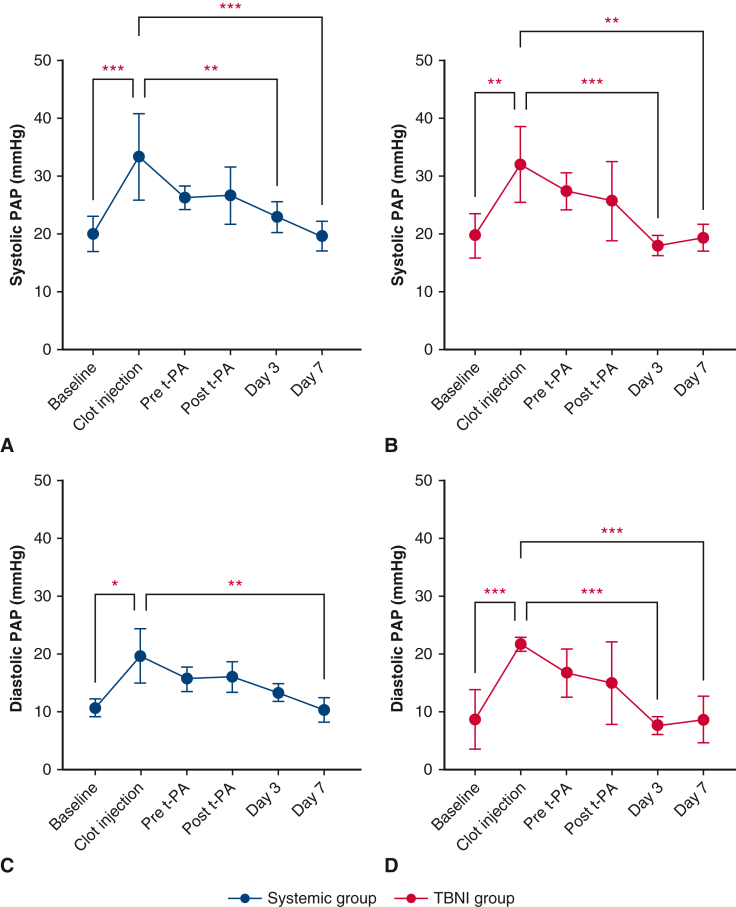
Objective: Endobronchial ultrasound-guided transbronchial needle injection (EBUS-TBNI) may effectively treat acute pulmonary embolisms (PEs). Here, we assessed the effectiveness of clot dissolution and safety of tissue plasminogen activator (t-PA) injection using EBUS-TBNI in a 1-week survival study of a porcine PE model.
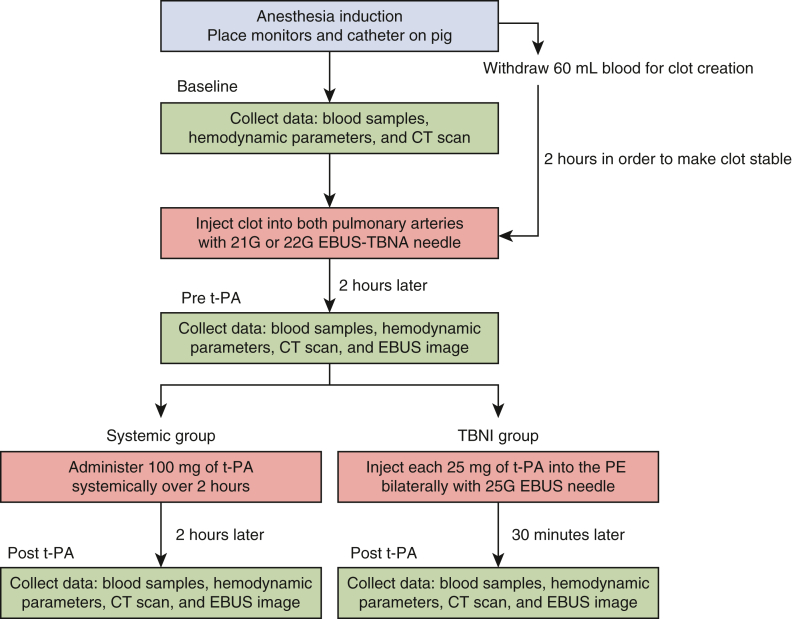
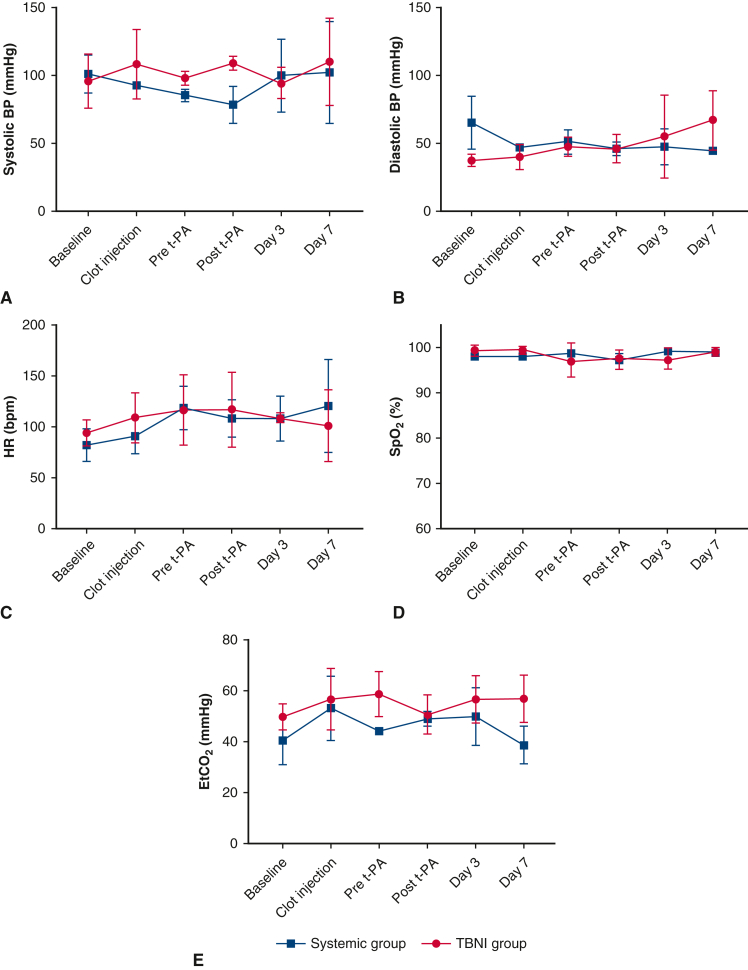
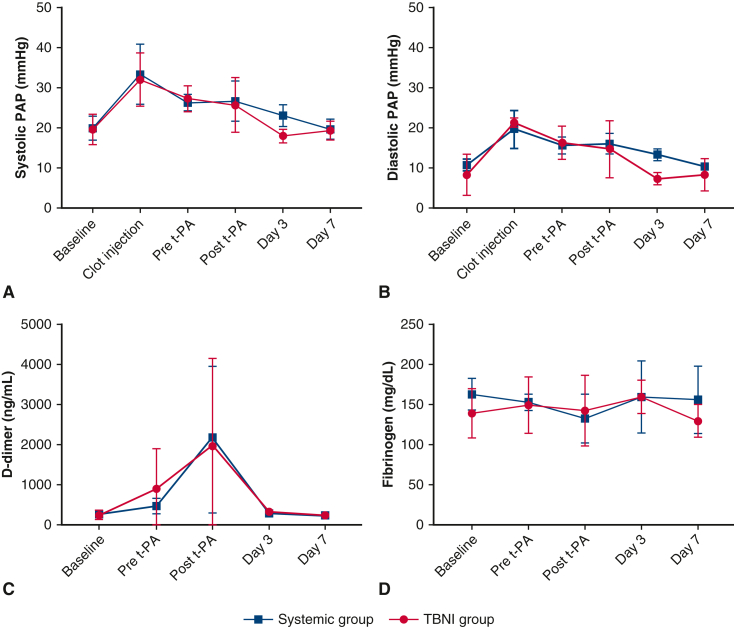
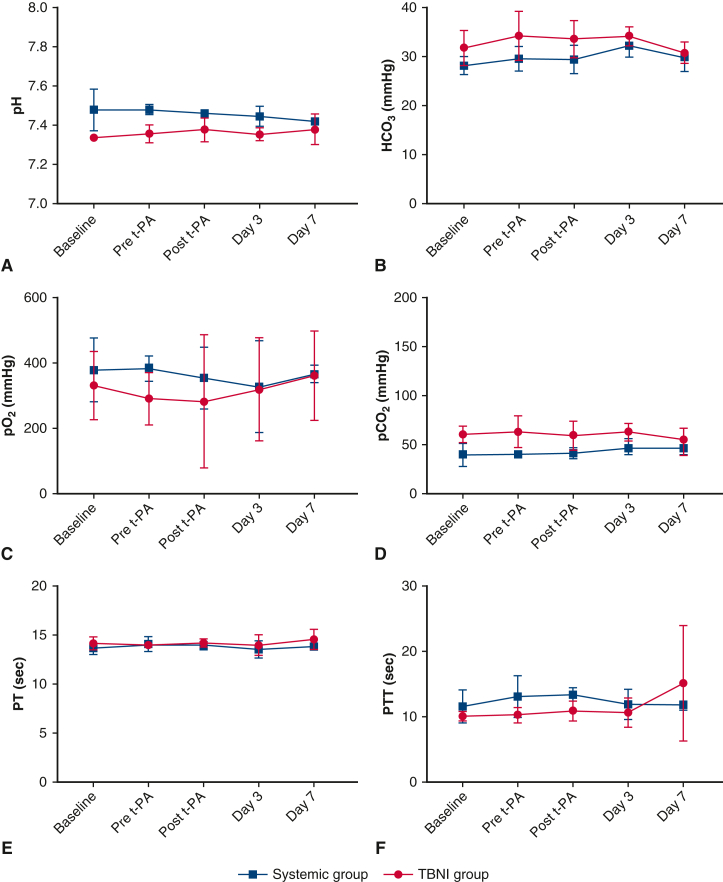
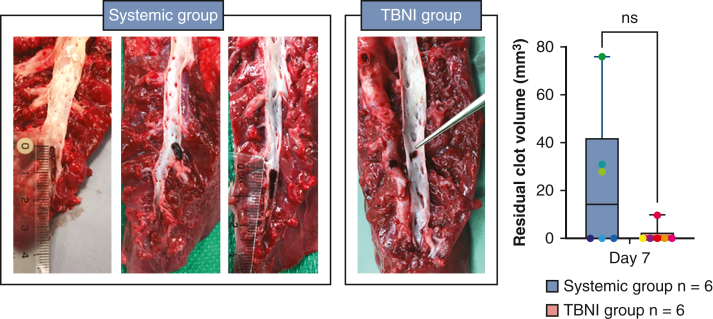
Methods: Six pigs with bilateral PEs were used: 3 for t-PA injection using EBUS-TBNI (TBNI group) and 3 for systemic administration of t-PA (systemic group). Once bilateral PEs were created, each 25 mg of t-PA injection using EBUS-TBNI for bilateral PEs (a total of 50 mg t-PA) and 100 mg of t-PA systemic administration was performed on day 1. Hemodynamic parameters, blood tests, and contrast-enhanced computed tomography scans were carried out at several time points. On day 7, pigs were humanely killed to evaluate the residual clot volume in the pulmonary arteries.
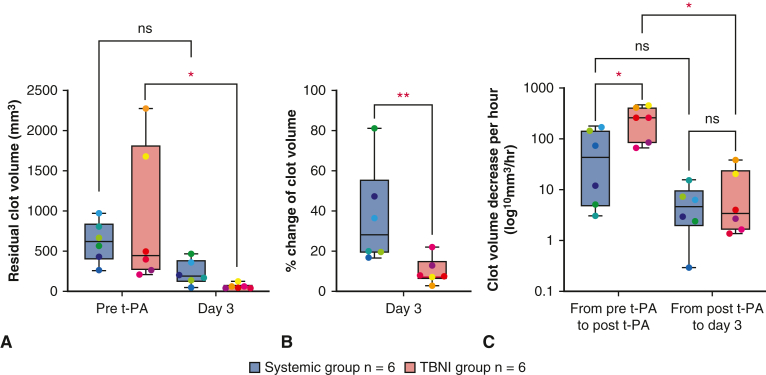
Results: The average of percent change of residual clot volumes was significantly lower in the TBNI group than in the systemic group (%: systemic group 36.6 ± 22.6 vs TBNI group 9.6 ± 6.1, P < .01) on day 3. Considering the elapsed time, the average decrease of clot volume per hour at pre-t-PA to post t-PA was significantly greater in the TBNI group than in the systemic group (mm3/hour: systemic 68.1 ± 68.1 vs TBNI 256.8 ± 148.1, P < .05). No hemorrhage was observed intracranially, intrathoracically, or intraperitoneally on any contrast-enhanced computed tomography images.
Conclusions: This study revealed that t-PA injection using EBUS-TBNI is an effective and safe way to dissolve clots.
Keywords: endobronchial ultrasound; preclinical animal model; pulmonary embolism; thrombolysis; transbronchial needle injection.
© 2023 The Author(s).
Conflict of interest statement
K.Y. received industry sponsored grants from the Olympus Corporation, Johnson & Johnson, and ODS Medical Inc. K.Y. is a consultant for Olympus Medical Corporation, Johnson & Johnson, and Medtronic. K.Y. has research collaborations with Siemens, Zidan Medical Inc, and OKF Technology. K.Y. is on the advisory board for Olympus American Inc, Medtronic, and Johnson & Johnson. All other authors reported no conflicts of interest. The Journal policy requires editors and reviewers to disclose conflicts of interest and to decline handling or reviewing manuscripts for which they may have a conflict of interest. The editors and reviewers of this article have no conflicts of interest.
Figures
Similar articles
-
Thrombolysis of Pulmonary Emboli via Endobronchial Ultrasound-Guided Transbronchial Needle Injection.Ann Thorac Surg. 2021 Aug;112(2):395-404. doi: 10.1016/j.athoracsur.2020.08.043. Epub 2020 Oct 24. Ann Thorac Surg. 2021. PMID: 33941356
-
Optimization of thrombolytic dose for treatment of pulmonary emboli using endobronchial ultrasound-guided transbronchial needle injection.J Thorac Cardiovasc Surg. 2023 May;165(5):e210-e221. doi: 10.1016/j.jtcvs.2022.08.044. Epub 2022 Sep 14. J Thorac Cardiovasc Surg. 2023. PMID: 36210209
-
Development of a minimally invasive pulmonary porcine embolism model via endobronchial ultrasound.J Thorac Dis. 2022 Feb;14(2):238-246. doi: 10.21037/jtd-21-1242. J Thorac Dis. 2022. PMID: 35280485 Free PMC article.
-
Convex probe endobronchial ultrasound: applications beyond conventional indications.J Thorac Dis. 2015 Sep;7(9):E289-97. doi: 10.3978/j.issn.2072-1439.2015.09.23. J Thorac Dis. 2015. PMID: 26543618 Free PMC article. Review.
-
Recent advances in convex probe endobronchial ultrasound: a narrative review.Ann Transl Med. 2021 Mar;9(5):419. doi: 10.21037/atm-21-225. Ann Transl Med. 2021. PMID: 33842640 Free PMC article. Review.
Cited by
-
Endobronchial Ultrasound Access to Pulmonary Vasculature in Thoracic Malignancy.Cancers (Basel). 2025 Feb 11;17(4):616. doi: 10.3390/cancers17040616. Cancers (Basel). 2025. PMID: 40002211 Free PMC article. Review.
References
-
- Kearon C., Akl E.A., Comerota A.J., Prandoni P., Bounameaux H., Goldhaber S.Z., et al. Antithrombotic therapy for VTE disease: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest physicians evidence-based clinical practice guidelines. Chest. 2012;141:e419S–e496S. - PMC - PubMed
-
- Konstantinides S.V., Meyer G., Becattini C., Bueno H., Geersing G.J., Harjola V.P., et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS) Eur Heart J. 2020;41:543–603. - PubMed
-
- Stevens S.M., Woller S.C., Kreuziger L.B., Bounameaux H., Doerschug K., Geersing G.J., et al. Antithrombotic therapy for VTE disease: second update of the CHEST guideline and expert panel report. Chest. 2021;160:e545–e608. - PubMed
-
- Engelhardt T.C., Taylor A.J., Simprini L.A., Kucher N. Catheter-directed ultrasound-accelerated thrombolysis for the treatment of acute pulmonary embolism. Thromb Res. 2011;128:149–154. - PubMed
-
- Pei D.T., Liu J., Yaqoob M., Ahmad W., Bandeali S.S., Hamzeh I.R., et al. Meta-analysis of catheter directed ultrasound-assisted thrombolysis in pulmonary embolism. Am J Cardiol. 2019;124:1470–1477. - PubMed
LinkOut - more resources
Full Text Sources
