

Clinical characteristics and prognosis in patients with neuronal surface antibody-mediated autoimmune encephalitis: a single-center cohort study in China
- PMID: 38152405
- PMCID: PMC10751914
- DOI: 10.3389/fimmu.2023.1213532
Clinical characteristics and prognosis in patients with neuronal surface antibody-mediated autoimmune encephalitis: a single-center cohort study in China
Abstract
Objective: This retrospective observational study primarily aimed to analyse the clinical characteristics of patients with neuronal surface antibody-mediated autoimmune encephalitis (AE) in China and report their prognosis after immunotherapy.
Methods: Clinical characteristics, laboratory or imaging examinations, and treatment outcomes of 103 patients diagnosed with AE between 1 September 2014 and 31 December 2020 were collected. Univariate and multivariate logistic regression analyses were performed to determine the predictors of poor prognosis.
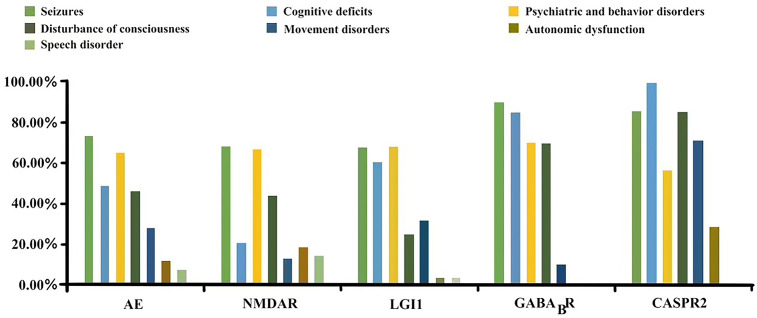
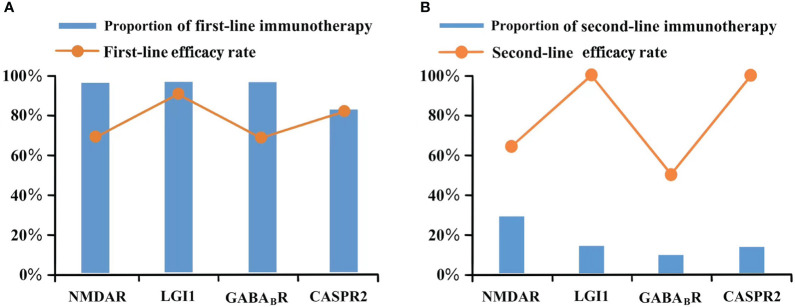
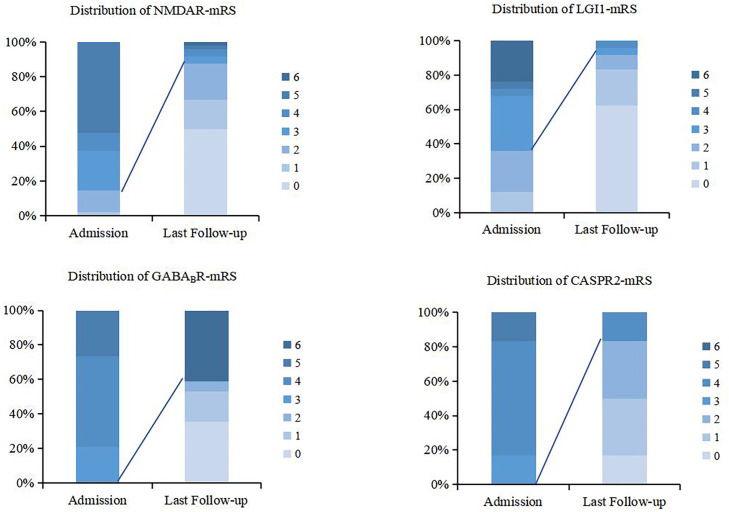
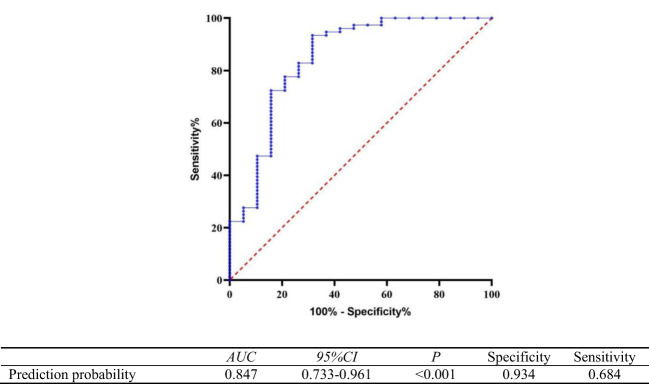
Results: Overall, 103 patients were enrolled in the study. The main clinical symptoms included seizures (74.8%), psychiatric and behavior disorders (66.0%), cognitive deficits (51.5%), disturbances of consciousness (45.6%), and movement disorders/involuntary movements (26.2%). The distribution of clinical syndromes also differed for different AE subtypes. The efficacy rates of first-line immunotherapy for anti-NMDAR, anti-LGI1, anti-GABABR, and anti-CASPR2 encephalitis were 70.2%, 92.3%, 70%, and 83.3%, respectively, and rituximab was administered to 21 patients as second-line immunotherapy, including 14 patients with anti-NMDAR encephalitis, 4 with anti-LGI1 encephalitis, 2 with anti-GABABR encephalitis, and 1 with anti-CASPR2 encephalitis. Five patients with poor effect of the second-line treatment received bortezomib. According to the results of the last follow-up, 78 patients had a good prognosis (mRS 0-2), and 21 patients had a poor prognosis (mRS 3-6). The proportion of patients with a poor prognosis was significantly higher in anti-GABABR encephalitis compared to the other AE subtypes (p<0.001). Multivariate analysis indicated that elevated neutrophil-to-lymphocyte ratio (NLR) and tumour presence were independent risk factors for poor prognosis. The regression equation of the model was logit(P)=-3.480 + 0.318 NLR+2.434 with or without tumour (with assignment =1, without assignment =0). The prediction probability generated by the regression model equation was used as the independent variable for receiver operating curve (ROC) analysis. The results showed that the area under the curve (AUC) of the prediction probability was 0.847 (95% CI, 0.733-0.961; p < 0.001).
Conclusions: Different AE subtypes demonstrated different clinical symptom spectra throughout the disease stage. Anti-LGI1 encephalitis and anti-CASPR2 encephalitis were more sensitive to first-line and second-line treatments. Anti-GABABR encephalitis had the worst prognosis among the abovementioned subtypes. The regression equation constructed using NLR and tumour presence effectively predicted the poor prognosis.
Keywords: autoimmune encephalitis; clinical characteristics; immunotherapy; neutrophil-to-lymphocyte ratio; prognosis.
Copyright © 2023 Huang, Liu, Wang, Wang, Hao and Guo.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Clinical Characteristics and Short-Term Prognosis of Children With Antibody-Mediated Autoimmune Encephalitis: A Single-Center Cohort Study.Front Pediatr. 2022 Jul 8;10:880693. doi: 10.3389/fped.2022.880693. eCollection 2022. Front Pediatr. 2022. PMID: 35874583 Free PMC article.
-
Long-term seizure outcomes in patients with autoimmune encephalitis: A prospective observational registry study update.Epilepsia. 2022 Jul;63(7):1812-1821. doi: 10.1111/epi.17245. Epub 2022 Apr 16. Epilepsia. 2022. PMID: 35357695
-
Clinical Characteristics and Short-Term Prognosis of Autoimmune Encephalitis: A Single-Center Cohort Study in Changsha, China.Front Neurol. 2019 May 24;10:539. doi: 10.3389/fneur.2019.00539. eCollection 2019. Front Neurol. 2019. PMID: 31178819 Free PMC article.
-
Anti-LGI1, anti-GABABR, and Anti-CASPR2 encephalitides in Asia: A systematic review.Brain Behav. 2020 Oct;10(10):e01793. doi: 10.1002/brb3.1793. Epub 2020 Aug 12. Brain Behav. 2020. PMID: 32783406 Free PMC article.
-
Three phenotypes of anti-N-methyl-D-aspartate receptor antibody encephalitis in children: prevalence of symptoms and prognosis.Pediatr Neurol. 2014 Oct;51(4):542-9. doi: 10.1016/j.pediatrneurol.2014.04.030. Epub 2014 May 29. Pediatr Neurol. 2014. PMID: 25070939 Review.
Cited by
-
Clinical, Electroencephalogram and Imaging Characteristics of Patients With Anti-LGI1 Antibody Encephalitis: A Multicenter Cohort Study.CNS Neurosci Ther. 2025 May;31(5):e70414. doi: 10.1111/cns.70414. CNS Neurosci Ther. 2025. PMID: 40322833 Free PMC article.
-
Autoimmune and infectious encephalitis: development of a discriminative tool for early diagnosis and initiation of therapy.J Neurol. 2024 Dec;271(12):7583-7591. doi: 10.1007/s00415-024-12712-7. Epub 2024 Oct 5. J Neurol. 2024. PMID: 39368009 Free PMC article.
-
Clinical characteristics and outcomes of patients with antibody-related autoimmune encephalitis presenting with disorders of consciousness: A prospective cohort study.Immun Inflamm Dis. 2024 Sep;12(9):e70019. doi: 10.1002/iid3.70019. Immun Inflamm Dis. 2024. PMID: 39315845 Free PMC article.
-
Abnormal CSF-Specific OCBs in Neuronal Surface Antibody-Associated Autoimmune Encephalitis Differentiating from Viral Encephalitis.J Inflamm Res. 2025 Feb 17;18:2307-2316. doi: 10.2147/JIR.S504003. eCollection 2025. J Inflamm Res. 2025. PMID: 39991667 Free PMC article.
-
Efficacy of rituximab as second-line therapy for autoimmune encephalitis: A systematic review and meta-analysis.Heliyon. 2025 Jan 7;11(2):e41747. doi: 10.1016/j.heliyon.2025.e41747. eCollection 2025 Jan 30. Heliyon. 2025. PMID: 39882485 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources