

doi: 10.1055/s-0043-1774396.
eCollection 2023 Sep.
An Asymptomatic Posttraumatic Intracranial Epidermal Inclusion Cyst: Avoiding the Maslow Hammer
Affiliations
- PMID: 38152521
- PMCID: PMC10749840
- DOI: 10.1055/s-0043-1774396
Item in Clipboard
An Asymptomatic Posttraumatic Intracranial Epidermal Inclusion Cyst: Avoiding the Maslow Hammer
Asian J Neurosurg.
.
No abstract available
Conflict of interest statement
Conflict of Interest None declared.
Figures

(
A
) Plain computed tomography (CT) of the head from 2008 showing a 4 × 3 cm trilobed cystic structure occupying the right frontal lobe with associated frontal bone erosion suggestive of a long-standing pathology. (
B
) Plain CT of the head from 2020 showing the marginally increased 5.4 × 4.2 cm hypointense cystic lesion suggestive of a benign etiology.

(
A
) T1-weighted axial magnetic resonance imaging (MRI) of the brain from 2008 showing the hypointense intra-axial plus extra-axial cystic lesion. (
B
) T2-weighted axial MRI of the brain from 2008 showing the homogenous hyperintense multilobulated lesion with septations within. (
C
) Fluid-attenuated inversion recovery (FLAIR) coronal MRI of the brain showing the frontal intradiploic extension of the lesion with no perilesional edema.
(
A
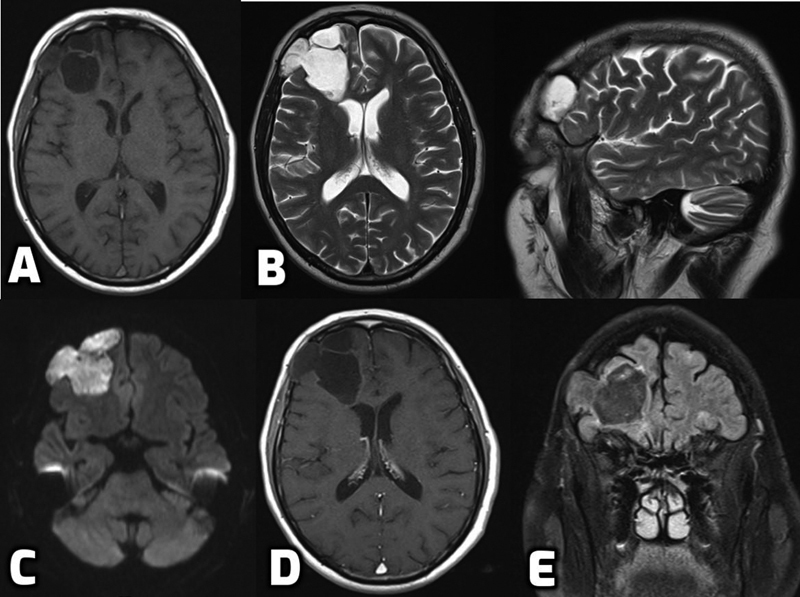
) T1-weighted axial magnetic resonance imaging (MRI) of the brain from 2020 showing the marginally increased hypointense cyst. (
B
) T2-weighted axial and sagittal MRI of the brain showing the homogenous multiseptated cyst with involvement of the frontal bone. (
C
) Diffusion-weighted MRI of the brain showing marked restriction within the lesion. (
D
) T1-weighted postcontrast axial MRI of the brain showing the absence of enhancement within the lesion. (
E
) Fluid-attenuated inversion recovery (FLAIR) coronal MRI of the brain denoting the intracerebral and extra-axial extension with no perilesional edema.

(
A
) T1-weighted axial magnetic resonance imaging (MRI) of the brain, (
B
) T2-weighted axial and sagittal, (
C
) diffusion-weighted image, (
D
) fluid-attenuated inversion recovery (FLAIR) coronal image, and (
E
) postcontrast axial and coronal images, from last follow-up showing no change in the characteristics of the lesion.
Similar articles
-
Posttraumatic epidermal inclusion cyst of the deep infratemporal fossa.Ann Plast Surg. 2001 Jan;46(1):68-71. doi: 10.1097/00000637-200101000-00015. Ann Plast Surg. 2001. PMID: 11192040
-
A Case of Digital Myxoid Cyst Coexisting with Epidermal Inclusion Cyst.Ann Dermatol. 2008 Jun;20(2):67-9. doi: 10.5021/ad.2008.20.2.67. Epub 2008 Jun 30. Ann Dermatol. 2008. PMID: 27303162 Free PMC article.
-
'To a man with a hammer, everything looks like a nail' (Abraham Maslow).ANZ J Surg. 2018 Sep;88(9):816-817. doi: 10.1111/ans.14757. ANZ J Surg. 2018. PMID: 30182416 No abstract available.
-
Epidermal inclusion cyst of the knee.Eur J Orthop Surg Traumatol. 2019 Aug;29(6):1355-1358. doi: 10.1007/s00590-019-02432-4. Epub 2019 Apr 9. Eur J Orthop Surg Traumatol. 2019. PMID: 30968204 Review.
-
Clitoral Epidermal Inclusion Cyst Leading to Anorgasmia: A Case Report and Literature Review.J Pediatr Adolesc Gynecol. 2020 Jun;33(3):321-323. doi: 10.1016/j.jpag.2020.01.150. Epub 2020 Feb 3. J Pediatr Adolesc Gynecol. 2020. PMID: 32028052 Review.
References
-
- Osborn A G, Preece M T. Intracranial cysts: radiologic-pathologic correlation and imaging approach. Radiology. 2006;239(03):650–664. - PubMed
-
- Fliedner E, Hinzpeter T. An intracranial epidermoid caused by trauma (author's transl) J Neurol. 1976;211(02):183–188. - PubMed
-
- Lee V S, Provenzale J M, Fuchs H E, Osumi A, McLendon R E. Post-traumatic epidermoid cyst: CT appearance. J Comput Assist Tomogr. 1995;19(01):153–155. - PubMed
-
- Green A J, Roberts D R, Swanson R A. Post-traumatic epidermoid cyst presenting with headache. Neurology. 2005;64(09):1657. - PubMed
LinkOut - more resources
Full Text Sources