

The Ponytail Lift: 22 Years of Experience in 600 Cases of Endoscopic Deep Plane Facial Rejuvenation
- PMID: 38152870
- PMCID: PMC11210079
- DOI: 10.1093/asj/sjad382
The Ponytail Lift: 22 Years of Experience in 600 Cases of Endoscopic Deep Plane Facial Rejuvenation
Abstract
Background: During aging, the face loses volume with progressive sagging of the soft tissues, while the neck demonstrates skin laxity and muscle banding. The treatment of facial and neck aging usually involves a traditional facelift, which can cause noticeable scarring and distortion of anatomy.
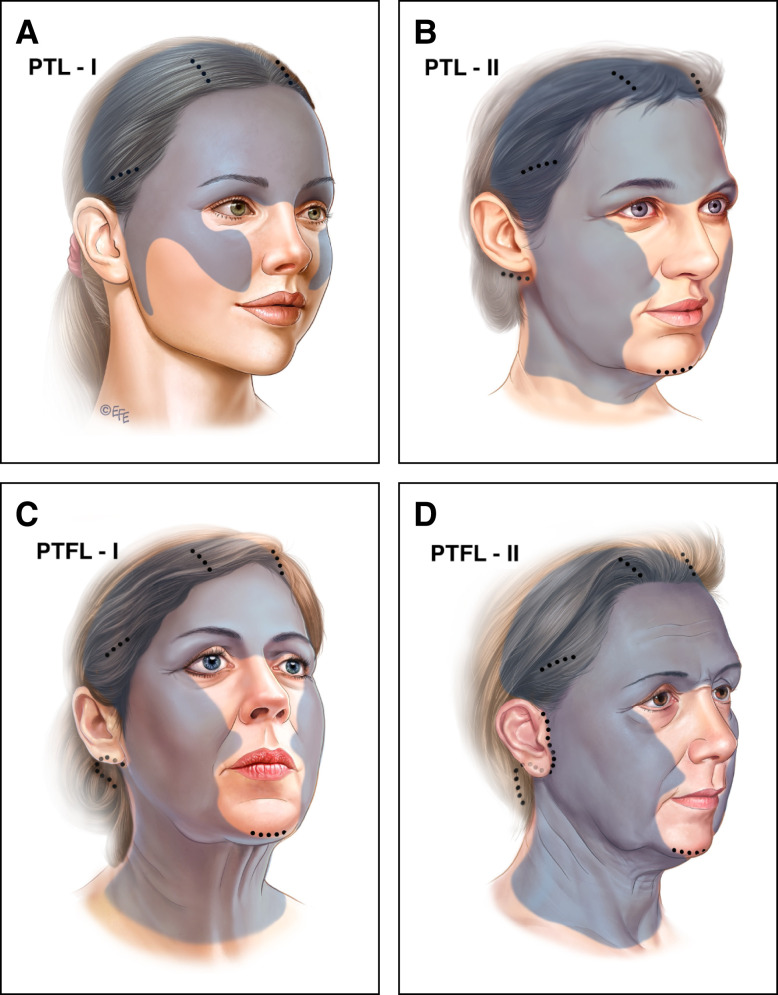
Objectives: Modern facelift surgery must avoid such shortcomings and still address aging in all layers of the face. To achieve this goal a novel surgical technique was developed and coined the "ponytail lift" (PTL). When global facial rejuvenation is indicated, this procedure is combined with neck skin excision and referred to as the "ponytail facelift" (PTFL).
Methods: A retrospective analysis of 600 consecutive cases over 22 years (2000-2022) of facial rejuvenation employing the endoscopic techniques of PTL and PTFL was performed. Patients were followed for at least 12 months postoperatively. Demographics, surgical data, and complications were recorded and analyzed. Additionally, technical details of the PTL and PTFL are discussed.
Results: There were no instances of postoperative skin flap necrosis, and no permanent nerve injuries were recorded. An additional surgical touch-up procedure to address unsatisfied aesthetic needs was performed in 20 cases.
Conclusions: The ponytail procedures offer a stepwise approach matched to the extent of the problem and are intended to refresh or transform the face with minimal incisions. The procedures represent a deep plane facelift without the scar burden, with incisions that are hidden in the temple, postauricular, and posterior scalp. The described techniques are safe and effective while providing reliable and satisfying results.
背景: 随着年龄的增长,面部体积会逐渐减小,软组织会逐渐下垂,而颈部会出现皮肤松弛和肌肉带状。面部和颈部衰老的治疗通常涉及传统的面部拉皮术,这会导致明显的疤痕和解剖结构扭曲。
目标: 现代面部拉皮手术必须避免此类缺点,同时还要解决面部所有层面的衰老问题。为了实现这一目标,开发了一种新颖的手术技术,创造了“马尾辫提升术”(PTL)这一名称。当需要进行整体面部年轻化时,该手术与颈部皮肤切除术相结合,称为“马尾辫拉皮术”(PTFL)。
方法: 回顾性分析了 22 年间(2000-2022 年)采用 PTL 和 PTFL 内窥镜技术进行面部年轻化的 600 个连续病例。术后对患者进行至少 12 个月的随访。记录并分析了人口统计学、手术数据和并发症。此外,还讨论了 PTL 和 PTFL 的技术细节。
结果: 没有出现术后皮瓣坏死的情况,也没有记录到永久性神经损伤。在 20 个病例中进行了额外的外科修补手术,以解决未满足的美学需求。
结论: 马尾辫手术提供了一种与问题程度相匹配的分步方法,旨在以最小的切口使面部得以改造或焕然一新。这些手术代表了一种深层平面拉皮术,没有疤痕负担,切口隐藏在太阳穴、耳后和头皮后部。所描述的技术是安全有效的,同时提供可靠且令人满意的结果。
证据等级:: 3 级(治疗性)
Level of Evidence: 3:

© The Author(s) 2023. Published by Oxford University Press on behalf of The Aesthetic Society.
Figures





Comment in
-
Commentary on: The Ponytail Lift: 22 Years of Experience in 600 Cases of Endoscopic Deep Plane Facial Rejuvenation.Aesthet Surg J. 2024 Jun 14;44(7):693-695. doi: 10.1093/asj/sjae017. Aesthet Surg J. 2024. PMID: 38290747 No abstract available.
-
Commentary on: The Ponytail Lift: 22 Years of Experience in 600 Cases of Endoscopic Deep Plane Facial Rejuvenation.Aesthet Surg J. 2024 Jun 14;44(7):696-698. doi: 10.1093/asj/sjae105. Aesthet Surg J. 2024. PMID: 38804276 No abstract available.
Similar articles
-
Advanced Endoscopic Techniques in Asian Facial Rejuvenation.Clin Plast Surg. 2023 Jan;50(1):51-60. doi: 10.1016/j.cps.2022.07.008. Clin Plast Surg. 2023. PMID: 36396261 Review.
-
The minimal access deep plane extended vertical facelift.Aesthet Surg J. 2011 Nov;31(8):874-90. doi: 10.1177/1090820X11424146. Aesthet Surg J. 2011. PMID: 22065880
-
Endoscopic-assisted face lift: review of 200 cases.Ann Plast Surg. 2004 Mar;52(3):234-9. doi: 10.1097/01.sap.0000110530.47141.0d. Ann Plast Surg. 2004. PMID: 15156974
-
Full SMAS: Endoscopy-Assisted Full Facial Rejuvenation.Aesthet Surg J. 2024 Nov 15;44(12):1247-1257. doi: 10.1093/asj/sjae177. Aesthet Surg J. 2024. PMID: 39133567
-
The deep-plane approach to neck rejuvenation.Facial Plast Surg Clin North Am. 2014 May;22(2):269-84. doi: 10.1016/j.fsc.2014.01.003. Facial Plast Surg Clin North Am. 2014. PMID: 24745388 Review.
Cited by
-
A Systematic Review and Comparative Analysis of Reconstructive Rhytidectomy: Advantages, Disadvantages, and Patient Outcomes.Cureus. 2024 Oct 7;16(10):e71006. doi: 10.7759/cureus.71006. eCollection 2024 Oct. Cureus. 2024. PMID: 39507149 Free PMC article. Review.
-
There Is No Facelift for All Seasons.Aesthet Surg J. 2024 Sep 16;44(10):1127-1129. doi: 10.1093/asj/sjae158. Aesthet Surg J. 2024. PMID: 39024417 Free PMC article. No abstract available.
-
Transtemporal Endoscopic Deep Plane Face Lift.Plast Reconstr Surg Glob Open. 2025 Jan 23;13(1):e6461. doi: 10.1097/GOX.0000000000006461. eCollection 2025 Jan. Plast Reconstr Surg Glob Open. 2025. PMID: 39850537 Free PMC article.
-
Current Trends in Facelift and Necklift Procedures.J Clin Med. 2025 Jun 16;14(12):4273. doi: 10.3390/jcm14124273. J Clin Med. 2025. PMID: 40566019 Free PMC article. Review.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
