

What Are the Recurrence Rates, Complications, and Functional Outcomes After Multiportal Arthroscopic Synovectomy for Patients With Knee Diffuse-type Tenosynovial Giant-cell Tumors?
- PMID: 38153106
- PMCID: PMC11219179
- DOI: 10.1097/CORR.0000000000002934
What Are the Recurrence Rates, Complications, and Functional Outcomes After Multiportal Arthroscopic Synovectomy for Patients With Knee Diffuse-type Tenosynovial Giant-cell Tumors?
Abstract
Background: Diffuse-type tenosynovial giant-cell tumor (D-TGCT), formerly known as pigmented villonodular synovitis, is a rare, locally aggressive, invasive soft tissue tumor that primarily occurs in the knee. Surgical excision is the main treatment option, but there is a high recurrence rate. Arthroscopic surgical techniques are emphasized because they are less traumatic and offer faster postoperative recovery, but detailed reports on arthroscopic techniques and outcomes of D-TGCT in large cohorts are still lacking.
Questions/purposes: (1) What is the recurrence rate of knee D-TGCT after multiportal arthroscopic synovectomy? (2) What are the complications, knee ROM, pain score, and patient-reported outcomes for patients, and do they differ between patients with and without recurrence? (3) What factors are associated with recurrence after arthroscopic treatment in patients with D-TGCT?
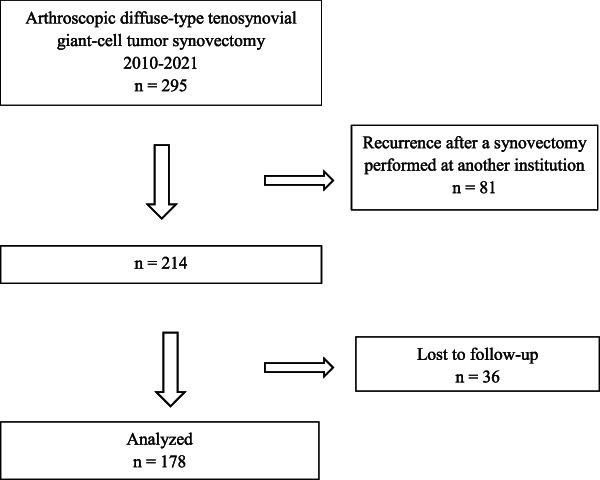
Methods: In this single-center, retrospective study conducted between January 2010 and April 2021, we treated 295 patients with knee D-TGCTs. We considered patients undergoing initial surgical treatment with multiportal arthroscopic synovectomy as potentially eligible. Based on that, 27% (81 of 295) of patients were excluded because of recurrence after synovectomy performed at another institution. Of the 214 patients who met the inclusion criteria, 17% (36 of 214) were lost to follow-up, leaving 83% (178 of 214) of patients in the analysis. Twenty-eight percent (50 of 178) of patients were men and 72% (128 of 178) were women, with a median (range) age of 36 years (7 to 69). The median follow-up duration was 80 months (26 to 149). All patients underwent multiportal (anterior and posterior approaches) arthroscopic synovectomy, and all surgical protocols were determined by discussion among four surgeons after preoperative MRI. A combined open posterior incision was used for patients with lesions that invaded or surrounded the blood vessels and nerves or invaded the muscle space extraarticularly. Standard postoperative adjuvant radiotherapy was recommended for all patients with D-TGCT who had extraarticular and posterior compartment invasion; for patients with only anterior compartment invasion, radiotherapy was recommended for severe cases as assessed by the surgeons and radiologists based on preoperative MRI and intraoperative descriptions. Postoperative recurrence at 5 years was calculated using a Kaplan-Meier survivorship estimator. The WOMAC score (0 to 96, with higher scores representing a worse outcome; minimum clinically important difference [MCID] 8.5), the Lysholm knee score (0 to 100, with higher scores being better knee function; MCID 25.4), the VAS for pain (0 to 10, with higher scores representing more pain; MCID 2.46), and knee ROM were used to evaluate functional outcomes. Because we did not have preoperative patient-reported outcomes scores, we present data on the proportion of patients who achieved the patient-acceptable symptom state (PASS) for each of those outcome metrics, which were 14.6 of 96 points on the WOMAC, 52.5 of 100 points on the Lysholm, and 2.32 of 10 points on the VAS.
Results: The symptomatic or radiographically documented recurrence at 5 years was 12% (95% confidence interval [CI] 7% to 17%) using the Kaplan-Meier estimator, with a mean recurrence time of 33 ± 19 months. Of these, three were asymptomatic recurrences found during regular MRI reviews, and the remaining 19 underwent repeat surgery. There was one intraoperative complication (vascular injury) with no effect on postoperative limb function and eight patients with postoperative joint stiffness, seven of whom improved with prolonged rehabilitation and one with manipulation under anesthesia. No postradiotherapy complications were found. The proportion of patients who achieved the preestablished PASS was 99% (176 of 178) for the VAS pain score, 97% (173 of 178) for the WOMAC score, and 100% (178 of 178) for the Lysholm score. A lower percentage of patients with recurrence achieved the PASS for WOMAC score than patients without recurrence (86% [19] versus 99% [154], OR 0.08 [95% CI 0.01 to 0.52]; p = 0.01), whereas no difference was found in the percentage of VAS score (95% [21] versus 99% [155], OR 0.14 [95% CI 0.01 to 2.25]; p = 0.23) or Lysholm score (100% [22] versus 100% [156], OR 1 [95% CI 1 to 1]; p = 0.99). Moreover, patients in the recurrence group showed worse knee flexion (median 135° [100° to 135°] versus median 135° [80° to 135°]; difference of medians 0°; p = 0.03), worse WOMAC score (median 3.5 [0 to 19] versus median 1 [0 to 29]; difference of medians 2.5; p = 0.01), and higher VAS pain score (median 1 [0 to 4] versus median 0 [0 to 4]; difference of medians 1; p < 0.01) than those in the nonrecurrence group, although no differences reached the MCID. No factors were associated with D-TGCT recurrence, including the use of postoperative radiotherapy, surgical technique, and invasion extent.
Conclusion: This single-center, large-cohort retrospective study confirmed that multiportal arthroscopic surgery can be used to treat knee D-TGCTs with a low recurrence rate, few complications, and satisfactory postoperative outcomes. Surgeons should conduct a thorough preoperative evaluation, meticulous arthroscopic synovectomy, and regular postoperative follow-up when treating patients with D-TGCT to reduce postoperative recurrence. Because the available evidence does not appear to fully support the use of postoperative adjuvant radiotherapy in all patients with D-TGCTs and our study design is inadequate to resolve this controversial issue, future studies should look for more appropriate indications for radiotherapy, such as planning based on a more precise classification of lesion invasion.
Level of evidence: Level III, therapeutic study.
Copyright © 2023 by the Association of Bone and Joint Surgeons.
Conflict of interest statement
Each author certifies that there are no funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article related to the author or any immediate family members. All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research® editors and board members are on file with the publication and can be viewed on request.
Figures
Similar articles
-
Surgical Hip Dislocation in the Era of Hip Arthroscopy Demonstrates High Survivorship and Improvements in Patient-reported Outcomes for Complex Femoroacetabular Impingement.Clin Orthop Relat Res. 2024 Sep 1;482(9):1671-1682. doi: 10.1097/CORR.0000000000003032. Epub 2024 Mar 21. Clin Orthop Relat Res. 2024. PMID: 38513108
-
Does Augmenting Irradiated Autografts With Free Vascularized Fibula Graft in Patients With Bone Loss From a Malignant Tumor Achieve Union, Function, and Complication Rate Comparably to Patients Without Bone Loss and Augmentation When Reconstructing Intercalary Resections in the Lower Extremity?Clin Orthop Relat Res. 2025 Jun 26. doi: 10.1097/CORR.0000000000003599. Online ahead of print. Clin Orthop Relat Res. 2025. PMID: 40569278
-
What Are the Complications, Function, and Survival of Tumor-devitalized Autografts Used in Patients With Limb-sparing Surgery for Bone and Soft Tissue Tumors? A Japanese Musculoskeletal Oncology Group Multi-institutional Study.Clin Orthop Relat Res. 2023 Nov 1;481(11):2110-2124. doi: 10.1097/CORR.0000000000002720. Epub 2023 Jun 14. Clin Orthop Relat Res. 2023. PMID: 37314384 Free PMC article.
-
Kinematic Alignment Does Not Result in Clinically Important Improvements After TKA Compared With Mechanical Alignment: A Meta-analysis of Randomized Trials.Clin Orthop Relat Res. 2025 Jun 1;483(6):1020-1030. doi: 10.1097/CORR.0000000000003356. Epub 2025 Jan 21. Clin Orthop Relat Res. 2025. PMID: 39842026
-
Does Minimally Invasive Surgery Provide Better Clinical or Radiographic Outcomes Than Open Surgery in the Treatment of Hallux Valgus Deformity? A Systematic Review and Meta-analysis.Clin Orthop Relat Res. 2023 Jun 1;481(6):1143-1155. doi: 10.1097/CORR.0000000000002471. Epub 2022 Nov 4. Clin Orthop Relat Res. 2023. PMID: 36332131 Free PMC article.
Cited by
-
Recurrence of arthroscopic treatment of pigmented villonodular synovitis of the knee: A systematic review and meta-analysis.J Exp Orthop. 2025 Feb 10;12(1):e70169. doi: 10.1002/jeo2.70169. eCollection 2025 Jan. J Exp Orthop. 2025. PMID: 39931151 Free PMC article. Review.
-
Multiportal Arthroscopy-assisted Surgical Resection of Diffuse-type Tenosynovial Giant Cell Tumors in the Ankle Joint Yields Favorable Clinical Outcomes: A Retrospective Study.Orthop Surg. 2024 Nov;16(11):2680-2687. doi: 10.1111/os.14180. Epub 2024 Aug 12. Orthop Surg. 2024. PMID: 39135389 Free PMC article.
-
Diffuse-Type Tenosynovial Giant Cell Tumor of the Knee: Clinical Course After Anterior Open Synovectomy.Curr Oncol. 2025 Jun 11;32(6):342. doi: 10.3390/curroncol32060342. Curr Oncol. 2025. PMID: 40558285 Free PMC article.
-
Tenosynovial giant cell tumor and its differential diagnosis in children.Pediatr Radiol. 2025 Jul 19. doi: 10.1007/s00247-025-06338-8. Online ahead of print. Pediatr Radiol. 2025. PMID: 40681854 Review.
References
-
- Bernthal NM, Ishmael CR, Burke ZDC. Management of pigmented villonodular synovitis (PVNS): an orthopedic surgeon's perspective. Curr Oncol Rep. 2020;22:63. - PubMed
-
- Blanco CE, Leon HO, Guthrie TB. Combined partial arthroscopic synovectomy and radiation therapy for diffuse pigmented villonodular synovitis of the knee. Arthroscopy. 2001;17:527-531. - PubMed
-
- Cassier PA, Gelderblom H, Stacchiotti S, et al. Efficacy of imatinib mesylate for the treatment of locally advanced and/or metastatic tenosynovial giant cell tumor/pigmented villonodular synovitis. Cancer. 2012;118:1649-1655. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
