

Preserflo TM MicroShunt implantation combined with Ologen TM in primary and secondary glaucoma patients in a clinical setting
- PMID: 38153975
- PMCID: PMC11001232
- DOI: 10.4103/IJO.IJO_1502_23
Preserflo TM MicroShunt implantation combined with Ologen TM in primary and secondary glaucoma patients in a clinical setting
Abstract
Purpose: This study aims to assess the effectiveness and safety of combining the Preserflo™ MicroShunt implant (MicroShunt) with a simultaneous Ologen™ implant in patients with glaucoma.
Methods: We conducted a retrospective study on consecutive patients with medically uncontrolled glaucoma who underwent MicroShunt + Ologen implantation as a standalone procedure or in combination with phacoemulsification (combined procedure). Success was defined as achieving an intraocular pressure (IOP) of 6-15 mmHg at 18 months post surgery, with a preoperative IOP reduction of at least 20%, and without (complete success) or with (qualified success) the need for antiglaucoma medications. The primary endpoint was the success rate.
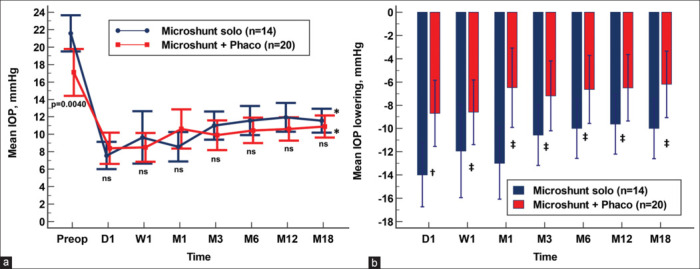
Results: Forty-eight eyes from 47 patients were included, with 28 eyes (58.3%) undergoing the standalone procedure and 20 eyes (41.7%) undergoing the combined procedure. Overall, there was a significant reduction in preoperative IOP from 19.7 ± 5.8 mmHg to 11.4 ± 2.6 mmHg at 18 months ( P < 0.0001). In the standalone procedure group, preoperative IOP decreased from 21.5 ± 5.2 mmHg to 11.7 ± 2.5 mmHg ( P < 0.0001), and in the combined procedure group, preoperative IOP decreased from 17.1 ± 5.8 mmHg to 10.9 ± 2.7 mmHg ( P = 0.0002), with no significant difference between the two groups regarding final IOP. The mean number of antiglaucoma medications significantly decreased from 3.2 ± 1.1 to 0.3 ± 0.7 in the overall study population ( P < 0.0001). At 18 months, 40 eyes (83.3%) were classified as successful. Regarding safety, out of the total number of eyes, two (4.2%) experienced choroidal detachment without visual impairment, two (4.2%) had transient hyphema, one (2.1%) showed reactivation of a corneal herpetic ulcer, one (2.1%) had diplopia, and one (2.1%) exhibited a shallow anterior chamber during the first week.
Conclusion: The combination of Ologen™ and Preserflo™ MicroShunt, either alone or in conjunction with phacoemulsification, demonstrated a favorable profile in terms of IOP reduction and safety.
Copyright © 2023 Copyright: © 2023 Indian Journal of Ophthalmology.
Conflict of interest statement
There are no conflicts of interest.
Figures




Similar articles
-
PreserFlo™ MicroShunt Combined with Phacoemulsification versus PreserFlo™ MicroShunt as a Standalone Procedure in Patients with Medically Resistant Open-Angle Glaucoma.J Curr Ophthalmol. 2022 Jul 26;34(2):180-186. doi: 10.4103/joco.joco_298_21. eCollection 2022 Apr-Jun. J Curr Ophthalmol. 2022. PMID: 36147269 Free PMC article.
-
Effectiveness of MicroShunt in Patients with Primary Open-Angle and Pseudoexfoliative Glaucoma: A Retrospective European Multicenter Study.Ophthalmol Glaucoma. 2022 Mar-Apr;5(2):210-218. doi: 10.1016/j.ogla.2021.08.005. Epub 2021 Aug 31. Ophthalmol Glaucoma. 2022. PMID: 34478904
-
Preliminary results of Preserflo Microshunt versus Preserflo Microshunt and Ologen implantation.Eye Vis (Lond). 2021 Sep 3;8(1):33. doi: 10.1186/s40662-021-00253-3. Eye Vis (Lond). 2021. PMID: 34479641 Free PMC article.
-
Comparing the safety and efficacy of Preserflo Microshunt implantation and trabeculectomy for glaucoma: A systematic review and meta-analysis.Acta Ophthalmol. 2024 Jun;102(4):e443-e451. doi: 10.1111/aos.16658. Epub 2024 Feb 20. Acta Ophthalmol. 2024. PMID: 38376121
-
Ab externo implantation of the MicroShunt, a poly (styrene-block-isobutylene-block-styrene) surgical device for the treatment of primary open-angle glaucoma: a review.Eye Vis (Lond). 2019 Nov 15;6:36. doi: 10.1186/s40662-019-0162-1. eCollection 2019. Eye Vis (Lond). 2019. PMID: 31807606 Free PMC article. Review.
Cited by
-
Xen 63 versus Preserflo MicroShunt implant in patients with primary open-angle glaucoma.Sci Rep. 2025 Jan 10;15(1):1634. doi: 10.1038/s41598-024-81616-3. Sci Rep. 2025. PMID: 39794378 Free PMC article.
References
-
- Joshi AB, Parrish RK, 2nd, Feuer WF. 2002 survey of the American Glaucoma Society: Practice preferences for glaucoma surgery and antifibrotic use. J Glaucoma. 2005;14:172–4. - PubMed
-
- Saheb H, Ahmed II. Micro-invasive glaucoma surgery: current perspectives and future directions. Curr Opin Ophthalmol. 2012;23:96–104. - PubMed
-
- Jampel HD, Musch DC, Gillespie BW, Lichter PR, Wright MM, Guire KE, et al. Perioperative complications of trabeculectomy in the collaborative initial glaucoma treatment study (CIGTS) Am J Ophthalmol. 2005;140:16–22. - PubMed
-
- Gedde SJ, Feuer WJ, Lim KS, Barton K, Goyal S, Ahmed IIK, et al. Treatment outcomes in the primary tube versus trabeculectomy study after 3 years of follow-up. Ophthalmology. 2020;127:333–45. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
