

Infarct-related structural disconnection and delirium in surgical aortic valve replacement patients
- PMID: 38155462
- PMCID: PMC10863920
- DOI: 10.1002/acn3.51949
Infarct-related structural disconnection and delirium in surgical aortic valve replacement patients
Abstract
Objective: Although acute brain infarcts are common after surgical aortic valve replacement (SAVR), they are often unassociated with clinical stroke symptoms. The relationship between clinically "silent" infarcts and in-hospital delirium remains uncertain; obscured, in part, by how infarcts have been traditionally summarized as global metrics, independent of location or structural consequence. We sought to determine if infarct location and related structural connectivity changes were associated with postoperative delirium after SAVR.
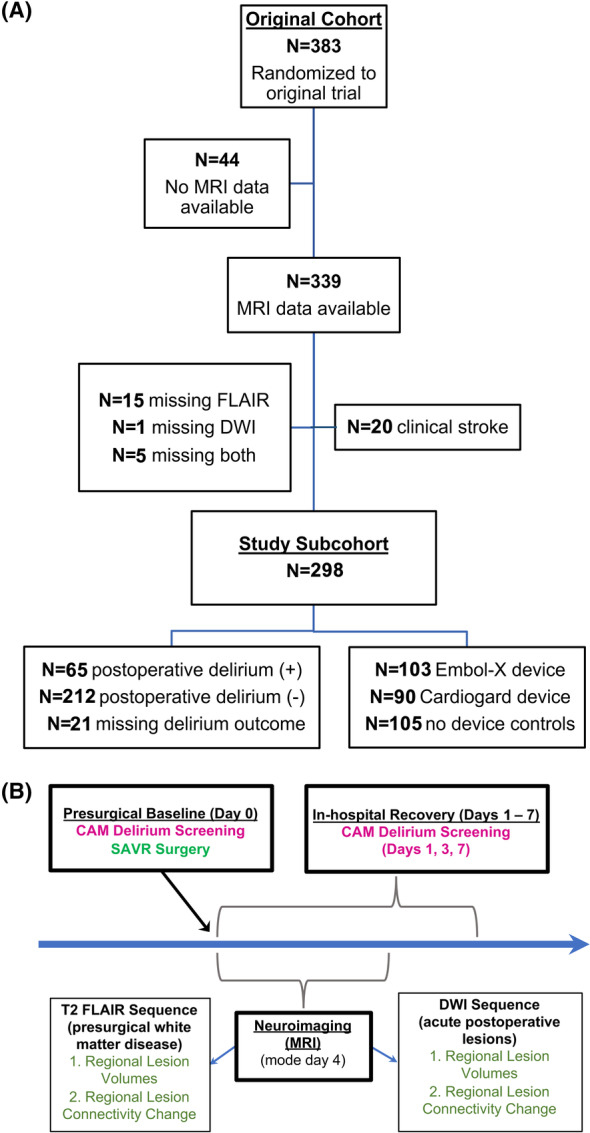
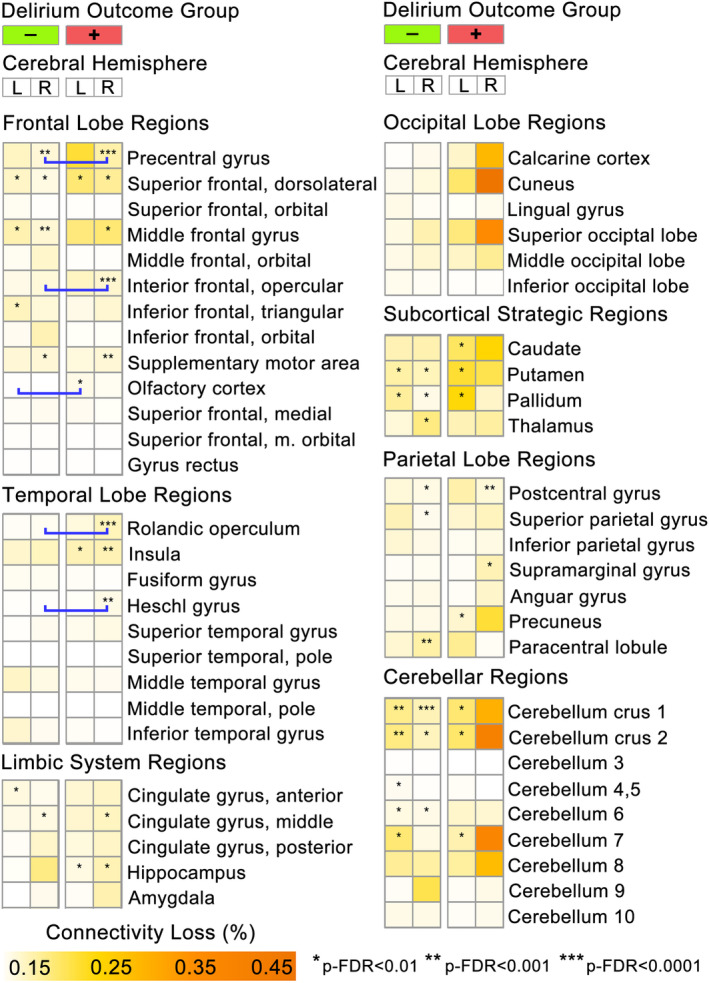
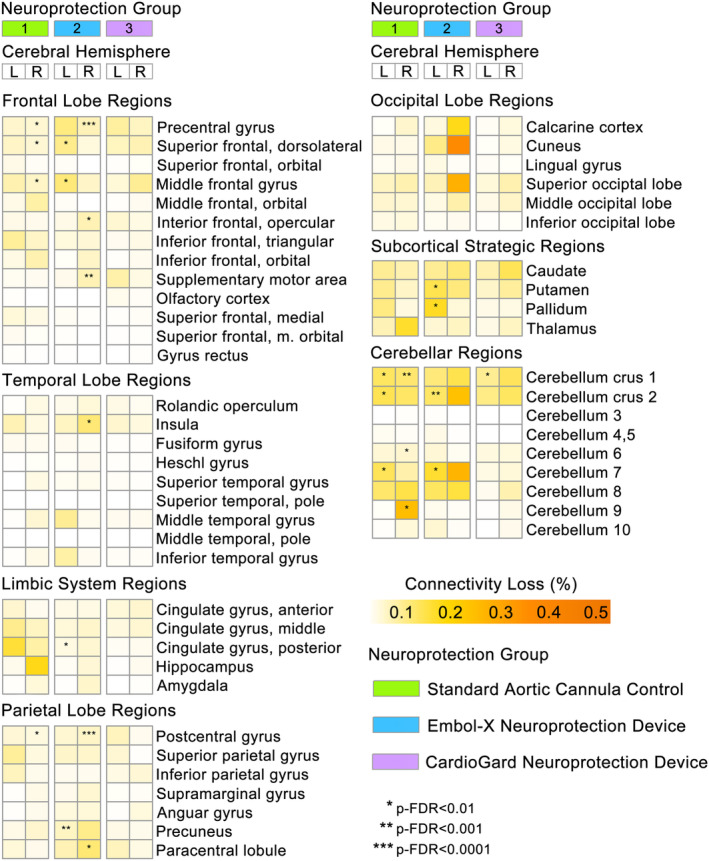
Methods: A secondary analysis of a randomized multicenter SAVR trial of embolic protection devices (NCT02389894) was conducted, excluding participants with clinical stroke or incomplete neuroimaging (N = 298; 39% female, 7% non-White, 74 ± 7 years). Delirium during in-hospital recovery was serially screened using the Confusion Assessment Method. Parcellation and tractography atlas-based neuroimaging methods were used to determine infarct locations and cortical connectivity effects. Mixed-effect, zero-inflated gaussian modeling analyses, accounting for brain region-specific infarct characteristics, were conducted to examine for differences within and between groups by delirium status and perioperative neuroprotection device strategy.
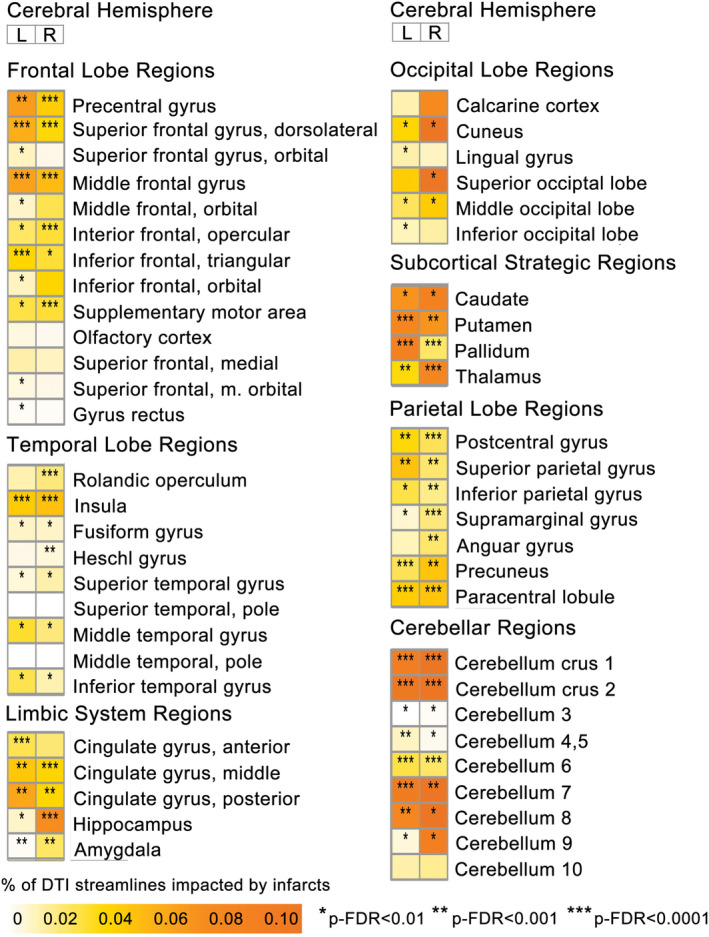
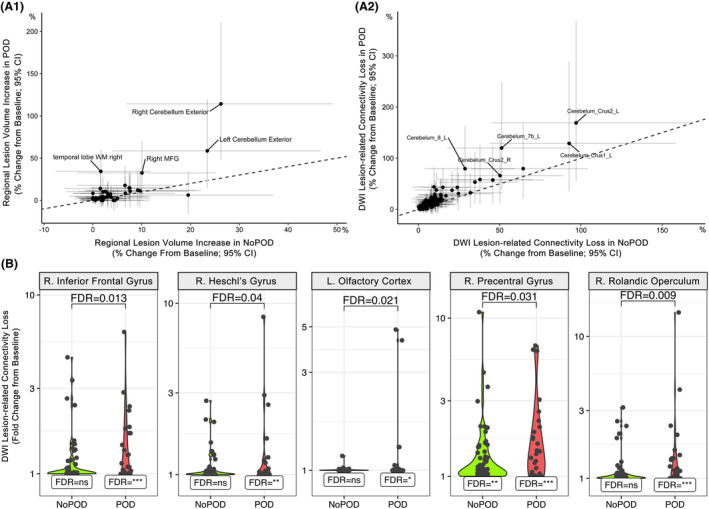
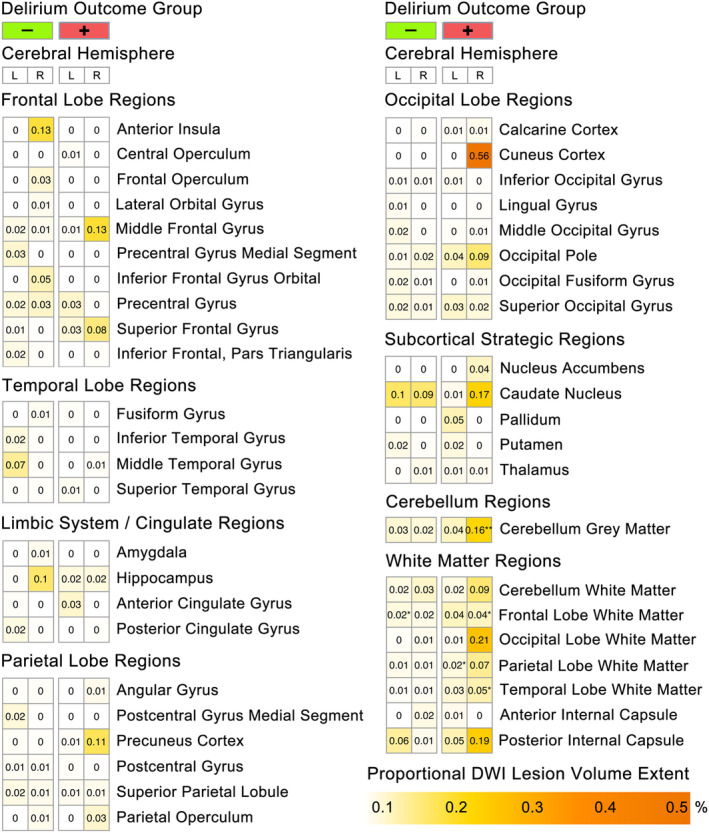
Results: 23.5% participants experienced postoperative delirium. Delirium was associated with significantly increased lesion volumes in the right cerebellum and temporal lobe white matter, while diffusion weighted imaging infarct-related structural disconnection (DWI-ISD) was observed in frontal and temporal lobe regions (p-FDR < 0.05). Fewer brain regions demonstrated DWI-ISD loss in the suction-based neuroprotection device group, relative to filtration-based device or standard aortic cannula.
Interpretation: Structural disconnection from acute infarcts was greater in patients who experienced postoperative delirium, suggesting that the impact from covert perioperative infarcts may not be as clinically "silent" as commonly assumed.
© 2023 The Authors. Annals of Clinical and Translational Neurology published by Wiley Periodicals LLC on behalf of American Neurological Association.
Conflict of interest statement
None of the authors have commercial relationships with the companies whose products were used in the study or may be affected by its outcomes.
Figures
References
-
- Stolz E, Gerriets T, Kluge A, Klovekorn WP, Kaps M, Bachmann G. Diffusion‐weighted magnetic resonance imaging and neurobiochemical markers after aortic valve replacement: implications for future neuroprotective trials? Stroke. 2004;35(4):888‐892. doi:10.1161/01.STR.0000120306.82787.5A - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
