

Resection rates and intention-to-treat outcomes in borderline and locally advanced pancreatic cancer: real-world data from a population-based, prospective cohort study (NORPACT-2)
- PMID: 38155512
- PMCID: PMC10755199
- DOI: 10.1093/bjsopen/zrad137
Resection rates and intention-to-treat outcomes in borderline and locally advanced pancreatic cancer: real-world data from a population-based, prospective cohort study (NORPACT-2)
Abstract
Background: Systemic chemotherapy is the initial treatment strategy for borderline resectable and locally advanced pancreatic cancer to facilitate curative resection. The aim of this study was to investigate the resection rates and overall survival in patients with borderline resectable pancreatic cancer and locally advanced pancreatic cancer.
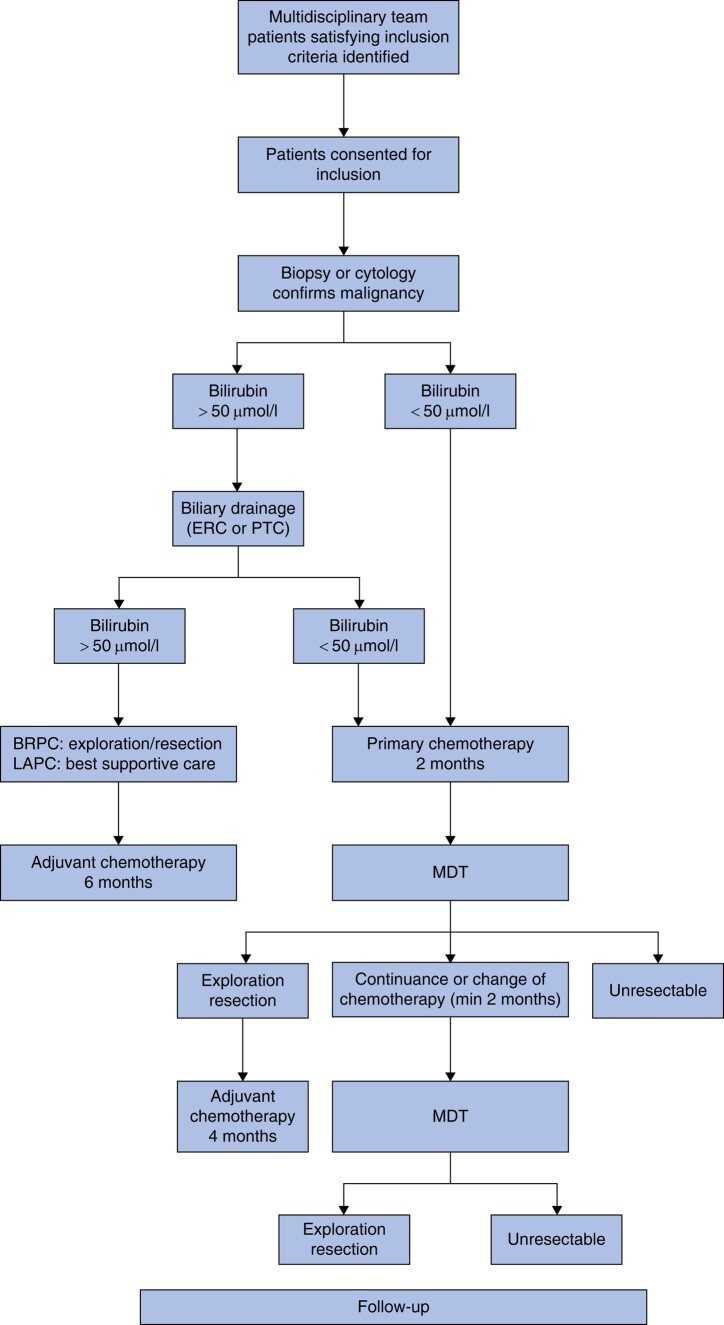
Methods: Consecutive patients with borderline resectable pancreatic cancer/locally advanced pancreatic cancer discussed by Oslo University Hospital multidisciplinary team between 2018 and 2020, serving a population of 3.1 million within a geographically defined area in south-eastern Norway, were included in this prospective Norwegian Pancreatic Cancer Trial-2 study, according to intention-to-treat principles. The total number of patients with pancreatic cancer was sought from the Cancer Registry of Norway.
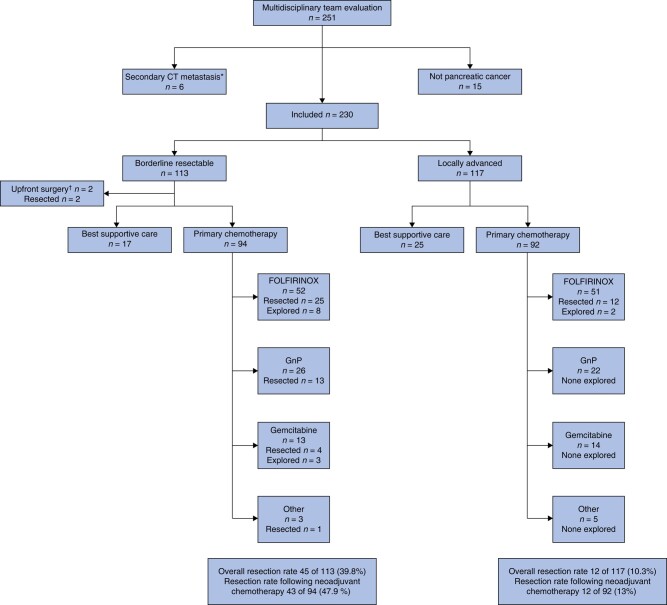
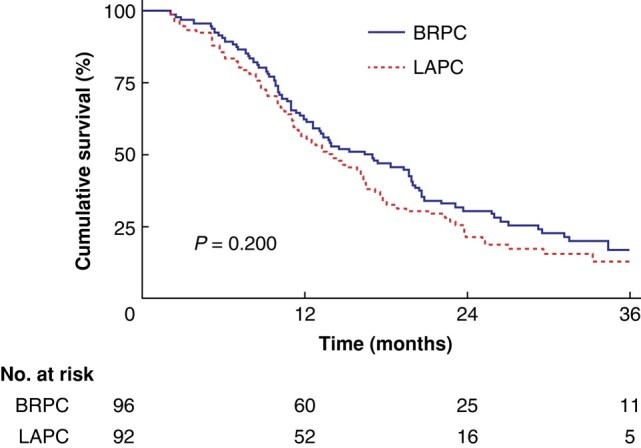
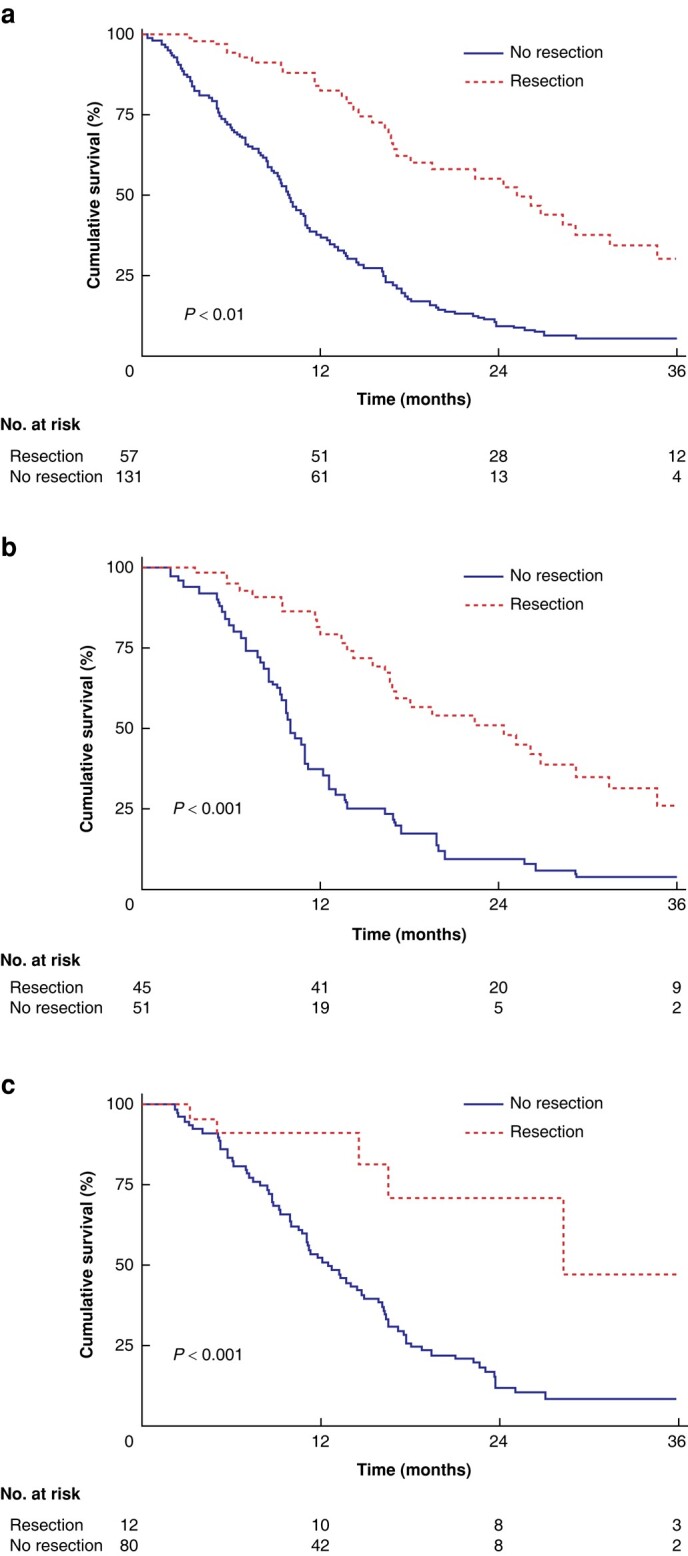
Results: A total of 1178 patients were diagnosed with pancreatic cancer, of whom 618 were referred to Oslo University Hospital. After multidisciplinary team evaluation, 230 patients were considered to have borderline resectable pancreatic cancer/locally advanced pancreatic cancer. The final study group consisted of 188 patients (borderline resectable pancreatic cancer n = 96, locally advanced pancreatic cancer n = 92) who were fit to receive primary chemotherapy. Resection rates were 46.9% (45 of 96) for borderline resectable pancreatic cancer and 13% (12 of 92) for locally advanced pancreatic cancer (P <0.001). Median overall survival was 14.6 months (borderline resectable pancreatic cancer 16.4 months; locally advanced pancreatic cancer 13.7 months, (P = 0.2)). Adjusted for immortal time bias, median overall survival for patients undergoing resection versus only chemotherapy was 24.4 months versus 10.1 months (P <0.001) for borderline resectable pancreatic cancer and 28.4 months versus 12.6 months for locally advanced pancreatic cancer (P = 0.001).
Conclusion: Resection rates and survival in patients with borderline resectable pancreatic cancer and locally advanced pancreatic cancer treated at a high-volume centre in a universal healthcare system compare well with those treated at international expert centres.Registration number: NCT04423731 (http://www.clinicaltrials.gov).
© The Author(s) 2023. Published by Oxford University Press on behalf of BJS Society Ltd.
Figures
Similar articles
-
Outcomes of Primary Chemotherapy for Borderline Resectable and Locally Advanced Pancreatic Ductal Adenocarcinoma.JAMA Surg. 2019 Oct 1;154(10):932-942. doi: 10.1001/jamasurg.2019.2277. JAMA Surg. 2019. PMID: 31339530 Free PMC article.
-
Intention to treat outcomes among patients with pancreatic cancer treated using International Study Group on Pancreatic Surgery recommended pathways for resectable and borderline resectable disease.ANZ J Surg. 2021 Jul;91(7-8):1549-1557. doi: 10.1111/ans.16643. Epub 2021 Feb 12. ANZ J Surg. 2021. PMID: 33576568
-
Surgical resection rates after neoadjuvant therapy for localized pancreatic ductal adenocarcinoma: meta-analysis.Br J Surg. 2022 Dec 13;110(1):34-42. doi: 10.1093/bjs/znac354. Br J Surg. 2022. PMID: 36346716
-
Postoperative complications after resection of borderline resectable and locally advanced pancreatic cancer: The impact of neoadjuvant chemotherapy with conventional radiation or stereotactic body radiation therapy.Surgery. 2018 May;163(5):1090-1096. doi: 10.1016/j.surg.2017.11.027. Epub 2018 Mar 12. Surgery. 2018. PMID: 29395234 Free PMC article.
-
Meta-analysis comparing upfront surgery with neoadjuvant treatment in patients with resectable or borderline resectable pancreatic cancer.Br J Surg. 2018 Jul;105(8):946-958. doi: 10.1002/bjs.10870. Epub 2018 Apr 30. Br J Surg. 2018. PMID: 29708592 Free PMC article. Review.
Cited by
-
Indole 3-acetate and response to therapy in borderline resectable or locally advanced pancreatic cancer.Front Oncol. 2024 Dec 20;14:1488749. doi: 10.3389/fonc.2024.1488749. eCollection 2024. Front Oncol. 2024. PMID: 39759130 Free PMC article.
-
ASO Author Reflections: From BRPC to LAPC-Rethinking Resectability in Pancreatic Cancer.Ann Surg Oncol. 2025 Jun 19. doi: 10.1245/s10434-025-17676-0. Online ahead of print. Ann Surg Oncol. 2025. PMID: 40537678 No abstract available.
-
REDISCOVER the change in surgical management of pancreatic cancer from anatomy to biology.Updates Surg. 2024 Sep;76(5):1569-1571. doi: 10.1007/s13304-024-01956-7. Epub 2024 Aug 16. Updates Surg. 2024. PMID: 39150628 No abstract available.
-
REDISCOVER International Guidelines on the Perioperative Care of Surgical Patients With Borderline-resectable and Locally Advanced Pancreatic Cancer.Ann Surg. 2024 Jul 1;280(1):56-65. doi: 10.1097/SLA.0000000000006248. Epub 2024 Feb 26. Ann Surg. 2024. PMID: 38407228 Free PMC article.
-
ASO Author Reflections: Population-Derived Outcome by Treatment-Intent for LAPC.Ann Surg Oncol. 2025 Jan;32(1):533-534. doi: 10.1245/s10434-024-16380-9. Epub 2024 Oct 25. Ann Surg Oncol. 2025. PMID: 39453586 Free PMC article. No abstract available.
References
-
- Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM, Matrisian LM. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res 2014;74:2913–2921 - PubMed
-
- Ducreux M, Cuhna AS, Caramella C, Hollebecque A, Burtin P, Goéré D et al. Cancer of the pancreas: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol 2015;26:v56–v68 - PubMed
-
- Neoptolemos JP, Kleeff J, Michl P, Costello E, Greenhalf W, Palmer DH. Therapeutic developments in pancreatic cancer: current and future perspectives. Nat Rev Gastroenterol Hepatol 2018;15:333–348 - PubMed
-
- Schneider M, Hackert T, Strobel O, Büchler MW. Technical advances in surgery for pancreatic cancer. Br J Surg 2021;108:777–785 - PubMed
-
- Helsedirektoratet . Nasjonalt Handlingsprogram Med Retningslinjer for Diagnostikk, Behandling og Oppfølging av Pancreaskreft. 2017; IS-2274. https://www.helsedirektoratet.no/retningslinjer/pancreaskreft-bukspyttkj...
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
