

Effect of Asymptomatic Common Carotid Artery Dissection on the Prognosis of Patients With Acute Type A Aortic Dissection
- PMID: 38156459
- PMCID: PMC10863841
- DOI: 10.1161/JAHA.123.031542
Effect of Asymptomatic Common Carotid Artery Dissection on the Prognosis of Patients With Acute Type A Aortic Dissection
Abstract
Background: Acute type A aortic dissection can extend upwards to involve the common carotid artery. However, whether asymptomatic common carotid artery dissection (CCAD) requires surgical repair remains controversial. This study aimed to explore the effect of asymptomatic CCAD without surgical intervention on the prognosis of patients who underwent surgery for acute type A aortic dissection.
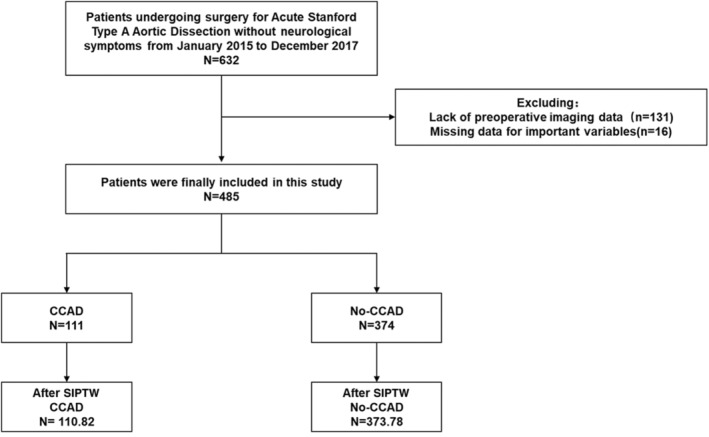
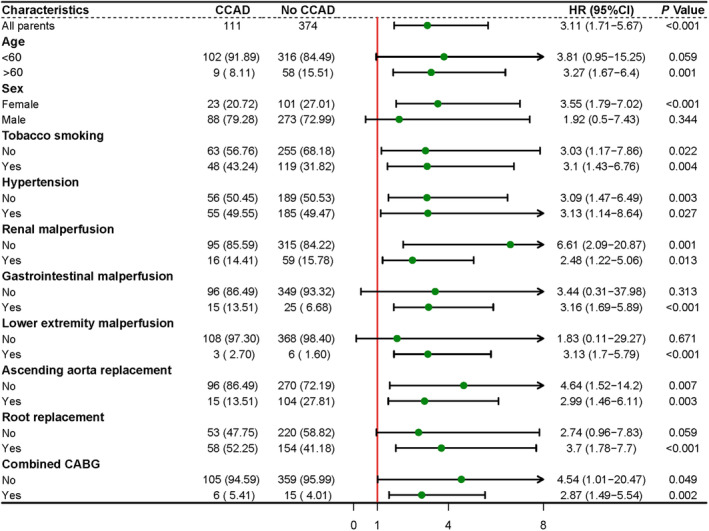
Methods and results: Between January 2015 and December 2017, 485 patients with no neurological symptoms who underwent surgery for acute type A aortic dissection were enrolled in this retrospective cohort study. The patients were divided into 2 groups based on the exposure factor of CCAD. CCAD was detected in 111 patients (22.9%), and after adjusting baseline data (standardized mean difference <0.1), the 30-day mortality (17.1% versus 6.0%, P<0.001) and incidence of fatal stroke (7.7% versus 1.6%, P=0.001) were significantly higher in the group with CCAD. Univariable and multivariable Cox regression analyses found CCAD as an independent risk factor for 30-day mortality (hazard ratio [HR], 2.8 [95% CI, 1.5-5.2]; P=0.001). At a median follow-up of 6.2 years (interquartile range, 5.6-6.9 years), landmark analysis with a cutoff value of 1 month postoperatively showed a significant increase in mortality in the group with CCAD, especially in the first month (log-rank P=0.002) and no significant difference in survival after the first month postoperatively between the 2 groups (log-rank P=0.955).
Conclusions: Asymptomatic CCAD increased the risk of early fatal stroke and death in patients with acute type A aortic dissection after surgery but did not affect midterm survival in patients who survived the early postoperative period.
Keywords: acute type a aortic dissection; cerebral malperfusion; common carotid artery dissection; prognosis.
Figures



References
-
- Isselbacher EM, Preventza O, Hamilton Black J 3rd, Augoustides JG, Beck AW, Bolen MA, Braverman AC, Bray BE, Brown‐Zimmerman MM, Chen EP, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022;146:e334–e482. doi: 10.1161/CIR.0000000000001106 - DOI - PMC - PubMed
-
- Pape LA, Awais M, Woznicki EM, Suzuki T, Trimarchi S, Evangelista A, Myrmel T, Larsen M, Harris KM, Greason K, et al. Presentation, diagnosis, and outcomes of acute aortic dissection: 17‐year trends from the International Registry of Acute Aortic Dissection. J Am Coll Cardiol. 2015;66:350–358. doi: 10.1016/j.jacc.2015.05.029 - DOI - PubMed
-
- Zindovic I, Gudbjartsson T, Ahlsson A, Fuglsang S, Gunn J, Hansson EC, Hjortdal V, Järvelä K, Jeppsson A, Mennander A, et al. Malperfusion in acute type A aortic dissection: an update from the Nordic Consortium for Acute Type A Aortic Dissection. J Thorac Cardiovasc Surg. 2019;157:1324–1333, e6. doi: 10.1016/j.jtcvs.2018.10.134 - DOI - PubMed
-
- Czerny M, Schoenhoff F, Etz C, Englberger L, Khaladj N, Zierer A, Weigang E, Hoffmann I, Blettner M, Carrel TP. The impact of pre‐operative malperfusion on outcome in acute type A aortic dissection: results from the GERAADA registry. J Am Coll Cardiol. 2015;65:2628–2635. doi: 10.1016/j.jacc.2015.04.030 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
