

Clinical phenogroup diversity and multiplicity: Impact on mechanisms of exercise intolerance in heart failure with preserved ejection fraction
- PMID: 38156712
- PMCID: PMC11096073
- DOI: 10.1002/ejhf.3105
Clinical phenogroup diversity and multiplicity: Impact on mechanisms of exercise intolerance in heart failure with preserved ejection fraction
Abstract
Aims: We aimed to clarify the extent to which cardiac and peripheral impairments to oxygen delivery and utilization contribute to exercise intolerance and risk for adverse events, and how this relates to diversity and multiplicity in pathophysiologic traits.
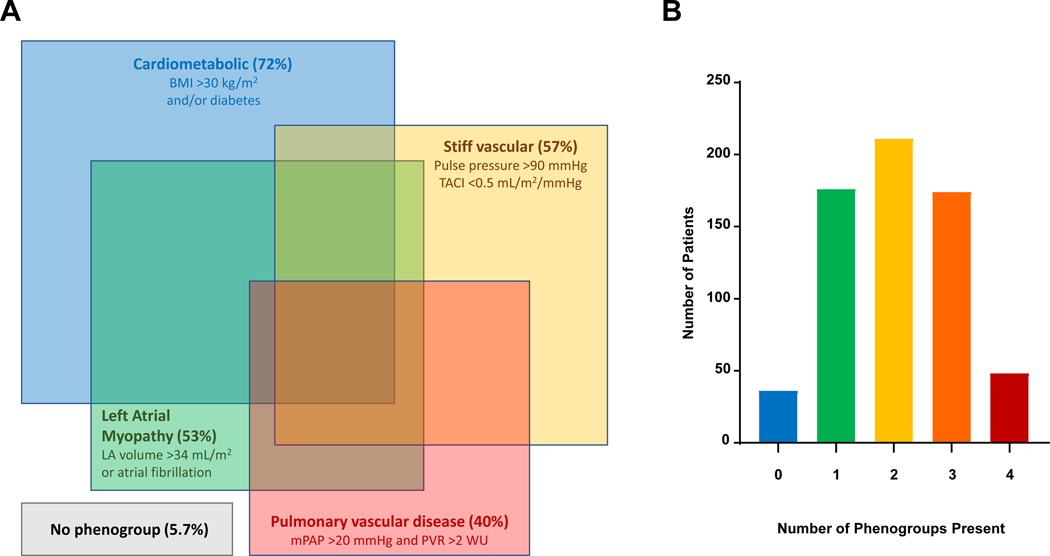
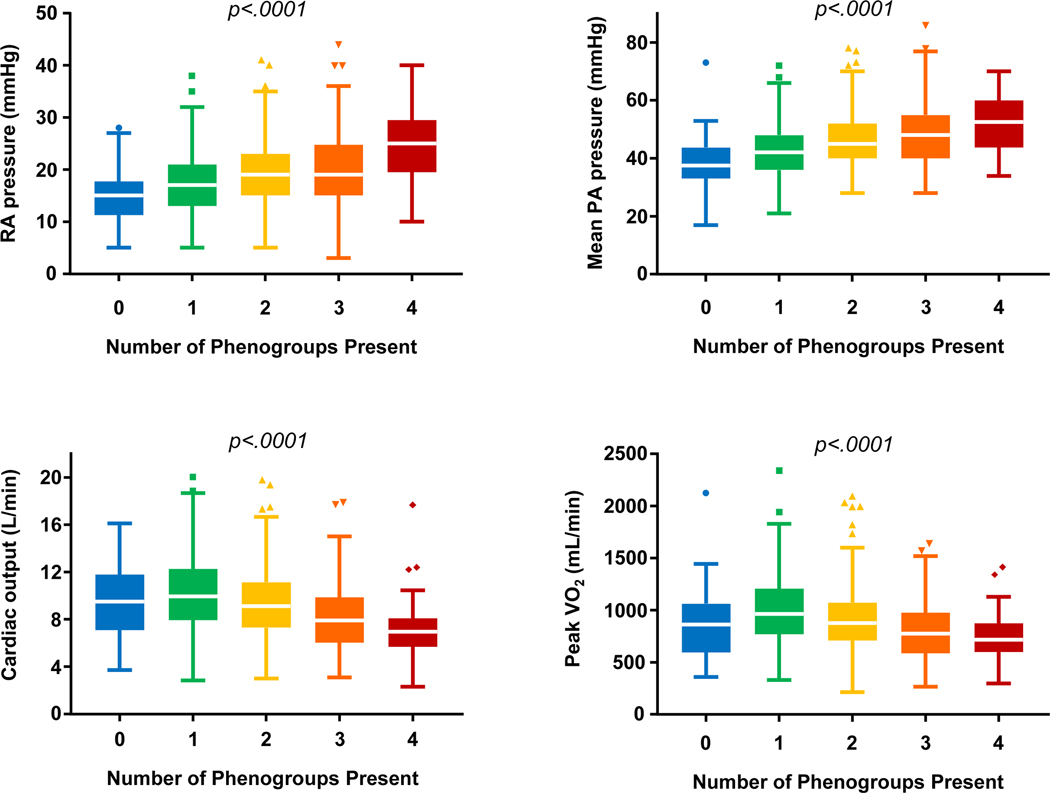
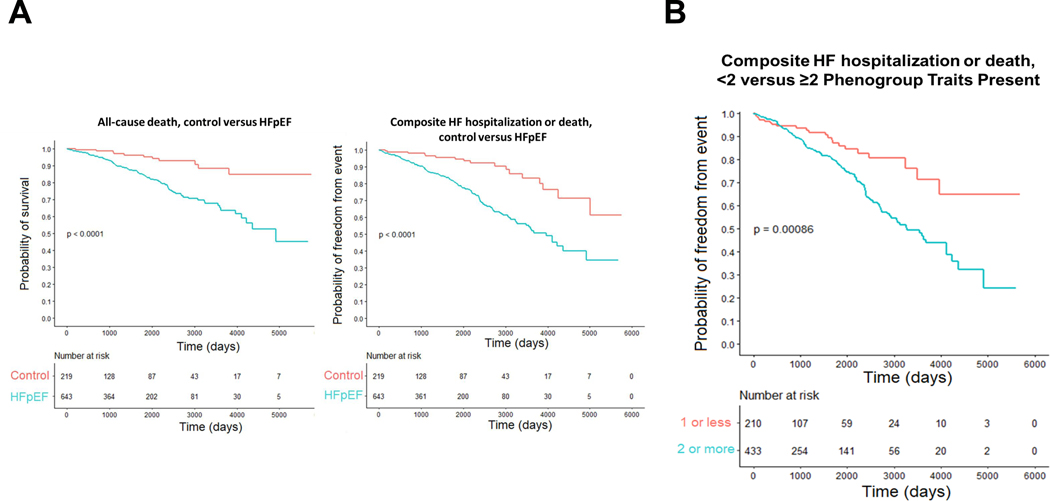
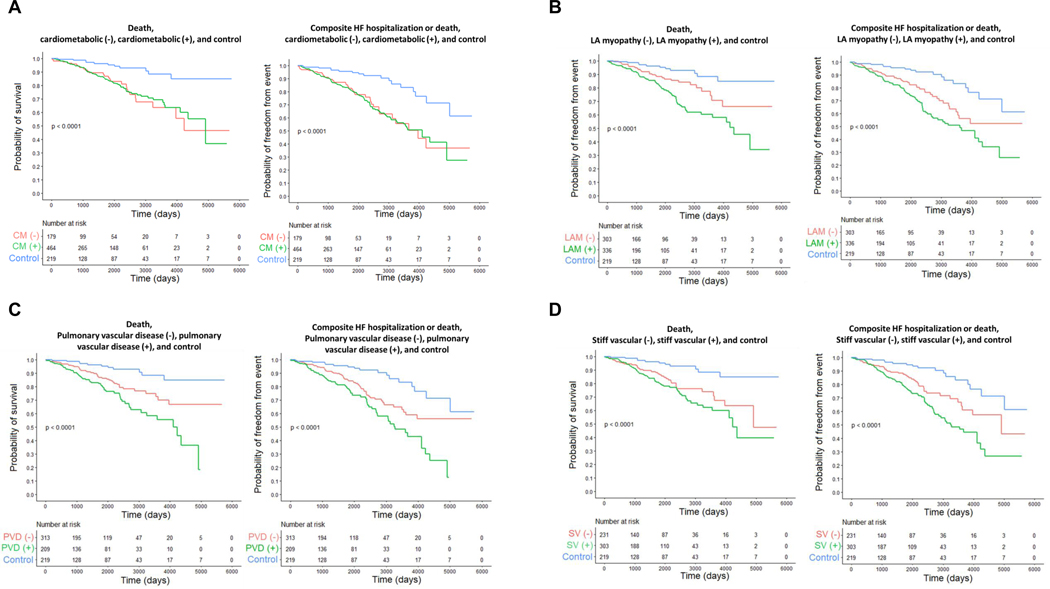
Methods and results: Individuals with heart failure with preserved ejection fraction (HFpEF) and non-cardiac dyspnoea (controls) underwent invasive cardiopulmonary exercise testing and clinical follow-up. Haemodynamics and oxygen transport responses were compared. HFpEF patients were then categorized a priori into previously-proposed, non-exclusive descriptive clinical trait phenogroups, including cardiometabolic, pulmonary vascular disease, left atrial myopathy, and vascular stiffening phenogroups based on clinical and haemodynamic profiles to contrast pathophysiology and clinical risk. Overall, patients with HFpEF (n = 643) had impaired cardiac output reserve with exercise (2.3 vs. 2.8 L/min, p = 0.025) and greater reliance on peripheral oxygen extraction augmentation (4.5 vs. 3.8 ml/dl, p < 0.001) compared to dyspnoeic controls (n = 219). Most (94%) patients with HFpEF met criteria for at least one clinical phenogroup, and 67% fulfilled criteria for multiple overlapping phenogroups. There was greater impairment in peripheral limitations in the cardiometabolic group and greater cardiac output limitations and higher pulmonary vascular resistance during exertion in the other phenogroups. Increasing trait multiplicity within a given patient was associated with worse exercise haemodynamics, poorer exercise capacity, lower cardiac output reserve, and greater risk for heart failure hospitalization or death (hazard ratio 1.74, 95% confidence interval 1.08-2.79 for 0-1 vs. ≥2 phenogroup traits present).
Conclusions: Though cardiac output response to exercise is limited in patients with HFpEF compared to those with non-cardiac dyspnoea, the relative contributions of cardiac and peripheral limitations vary with differing numbers and types of clinical phenotypic traits present. Patients fulfilling criteria for greater multiplicity and diversity of HFpEF phenogroup traits have poorer exercise capacity, worsening haemodynamic perturbations, and greater risk for adverse outcome.
Keywords: Exercise capacity; HFpEF; Heart failure; Outcome; Phenotype.
© 2023 European Society of Cardiology.
Conflict of interest statement
Figures
Similar articles
-
Exercise Stress Echocardiography-Based Phenotyping of Heart Failure With Preserved Ejection Fraction.J Am Soc Echocardiogr. 2024 Aug;37(8):759-768. doi: 10.1016/j.echo.2024.05.003. Epub 2024 May 15. J Am Soc Echocardiogr. 2024. PMID: 38754750
-
Clinical Phenogroups in Heart Failure With Preserved Ejection Fraction: Detailed Phenotypes, Prognosis, and Response to Spironolactone.JACC Heart Fail. 2020 Mar;8(3):172-184. doi: 10.1016/j.jchf.2019.09.009. Epub 2020 Jan 8. JACC Heart Fail. 2020. PMID: 31926856 Free PMC article. Clinical Trial.
-
Cardiac output response to exercise in relation to metabolic demand in heart failure with preserved ejection fraction.Eur J Heart Fail. 2013 Jul;15(7):776-85. doi: 10.1093/eurjhf/hft026. Epub 2013 Feb 20. Eur J Heart Fail. 2013. PMID: 23426022 Free PMC article.
-
Impaired Exercise Tolerance in Heart Failure With Preserved Ejection Fraction: Quantification of Multiorgan System Reserve Capacity.JACC Heart Fail. 2020 Aug;8(8):605-617. doi: 10.1016/j.jchf.2020.03.008. Epub 2020 Jun 10. JACC Heart Fail. 2020. PMID: 32535122 Free PMC article. Review.
-
Relative Impairments in Hemodynamic Exercise Reserve Parameters in Heart Failure With Preserved Ejection Fraction: A Study-Level Pooled Analysis.JACC Heart Fail. 2018 Feb;6(2):117-126. doi: 10.1016/j.jchf.2017.10.014. JACC Heart Fail. 2018. PMID: 29413366 Free PMC article. Review.
Cited by
-
IGF-1 levels in the general population, heart failure patients, and individuals with acromegaly: differences and projections from meta-analyses-a dual perspective.Front Cardiovasc Med. 2024 Oct 31;11:1379257. doi: 10.3389/fcvm.2024.1379257. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 39544311 Free PMC article.
-
Towards a phenotype profiling of the patients with heart failure and preserved ejection fraction.Eur Heart J Suppl. 2025 Feb 19;27(Suppl 1):i115-i121. doi: 10.1093/eurheartjsupp/suae095. eCollection 2025 Feb. Eur Heart J Suppl. 2025. PMID: 39980782 Free PMC article.
-
Diagnostic and therapeutic practice for HFpEF across continents and regions: An international survey.ESC Heart Fail. 2025 Feb;12(1):487-496. doi: 10.1002/ehf2.15084. Epub 2024 Oct 1. ESC Heart Fail. 2025. PMID: 39351634 Free PMC article.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
