

Distribution of regional lymph nodes metastasis in 870 cases of nasopharyngeal carcinoma and the suggestions for individualized elective prophylactic neck irradiation with intensity-modulated radiotherapy
- PMID: 38156901
- PMCID: PMC10905225
- DOI: 10.1002/cam4.6723
Distribution of regional lymph nodes metastasis in 870 cases of nasopharyngeal carcinoma and the suggestions for individualized elective prophylactic neck irradiation with intensity-modulated radiotherapy
Abstract
Purpose: To explore the feasibility of individualized elective prophylactic neck irradiation (iEPNI) for optimizing current approach by investigating metastatic lymph nodes (LNs) distribution in nasopharyngeal carcinoma (NPC).
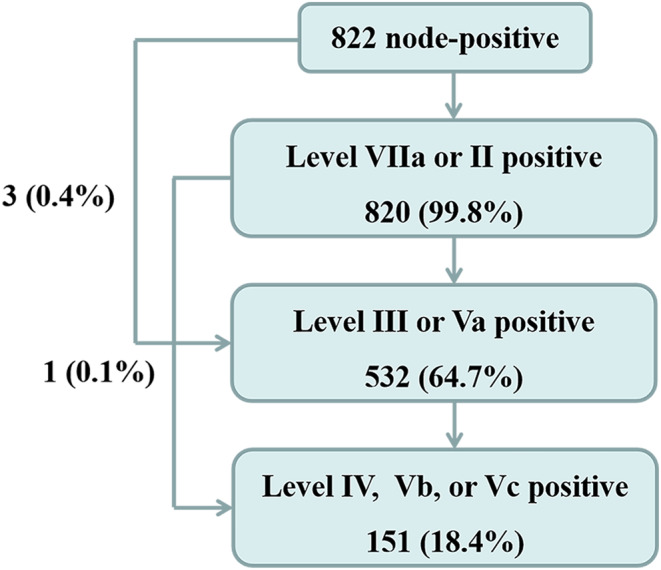
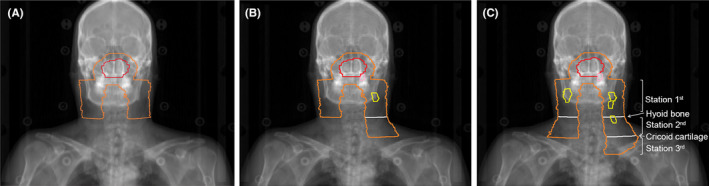
Materials and methods: Records of 870 NPC patients without distant metastasis in Hunan Cancer Hospital from January 2019 to December 2019 were reviewed. LNs' locations were identified based on the 2013 guidelines. The intra-regional lymphatic drainage (IRLD) areas included Station 1st (level VIIa and II), Station 2nd (level III and Va), and Station 3rd (level IV, Vb, and Vc). Other levels were categorized as extra-regional areas.
Results: Among the 870 patients, 94.5% cases exhibited LNs metastasis, including unilateral metastasis in 198 patients and bilateral metastasis in 624 patients. In the whole cohort, the most common involved IRLD areas were level IIb (87.1%), VIIa (80.0%), IIa (61.8%), Va (30.6%), IV (21.4%), Vb (8.9%), and Vc (1.1%). Besides, rates of LNs metastasis in Station 1st, 2nd, and 3rd were 94.3%, 61.1%, and 22.9%, respectively. Only four patients (4, 0.5%) revealed skipping metastasis among the three stations.
Conclusions: Lymph node metastasis follows an organized pattern from Station 1st to 3rd with scarce skipping metastasis. A potential iEPNI strategy of prophylactic neck irradiation to the ipsilateral latter node-negative station appears promising in NPC patients. Further prospective investigations are warranted to validate the approach.
Keywords: elective prophylactic neck irradiation; intensity-modulated radiotherapy; lymph nodes distribution; nasopharyngeal carcinoma.
© 2023 The Authors. Cancer Medicine published by John Wiley & Sons Ltd.
Conflict of interest statement
Not applicable.
Figures
References
-
- Pfister DG, Spencer S, Adkins D, et al. NCCN clinical practice guidelines in oncology (NCCN guidelines®). Head and Neck Cancers. 2023, Version 1. 2023. - PubMed
-
- Ou D, Blanchard P, El Khoury C, et al. Induction chemotherapy with docetaxel, cisplatin and fluorouracil followed by concurrent chemoradiotherapy or chemoradiotherapy alone in locally advanced non‐endemic nasopharyngeal carcinoma. Oral Oncol. 2016;62:114‐121. doi:10.1016/j.oraloncology.2016.10.011 - DOI - PubMed
-
- Sun X, Su S, Chen C, et al. Long‐term outcomes of intensity‐modulated radiotherapy for 868 patients with nasopharyngeal carcinoma: an analysis of survival and treatment toxicities. Radiother Oncol. 2014;110(3):398‐403. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
