

Do We Need to Administer Fludrocortisone in Addition to Hydrocortisone in Adult Patients With Septic Shock? An Updated Systematic Review With Bayesian Network Meta-Analysis of Randomized Controlled Trials and an Observational Study With Target Trial Emulation
- PMID: 38156911
- PMCID: PMC10930378
- DOI: 10.1097/CCM.0000000000006161
Do We Need to Administer Fludrocortisone in Addition to Hydrocortisone in Adult Patients With Septic Shock? An Updated Systematic Review With Bayesian Network Meta-Analysis of Randomized Controlled Trials and an Observational Study With Target Trial Emulation
Abstract
Objectives: This systematic review and Bayesian network meta-analysis evaluated the efficacy and safety of hydrocortisone combined with fludrocortisone or hydrocortisone alone, compared with placebo in adult patients with septic shock.
Data sources: By extending a prior Cochrane review, databases, including PubMed, Embase, the Cochrane Library, and ClinicalTrials.gov , along with other relevant websites, were searched until August 31, 2023.
Study selection: Randomized controlled trials (RCTs) and observational studies using target trial emulation were included.
Data extraction: The primary outcome was short-term mortality with an emphasis on 28- or 30-day mortality as the main measure and in-hospital or ICU mortality as the nearest surrogate of this measure. Three of the most common adverse events, namely, gastroduodenal bleeding, superinfection, and hyperglycemia, were also considered.
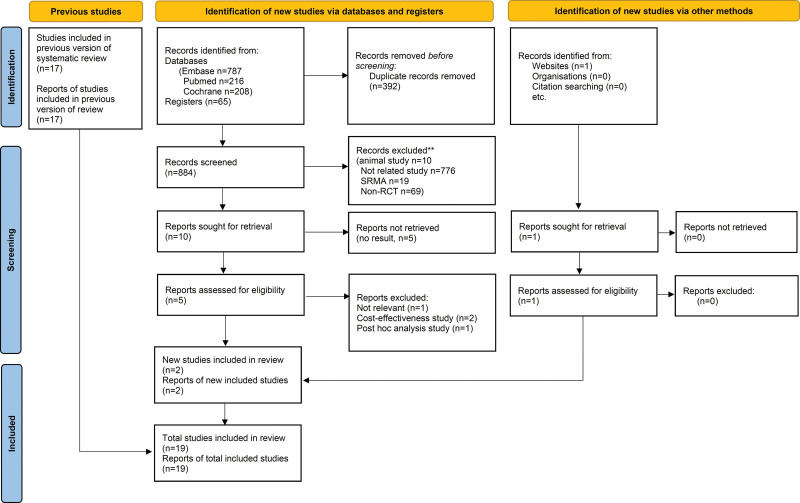
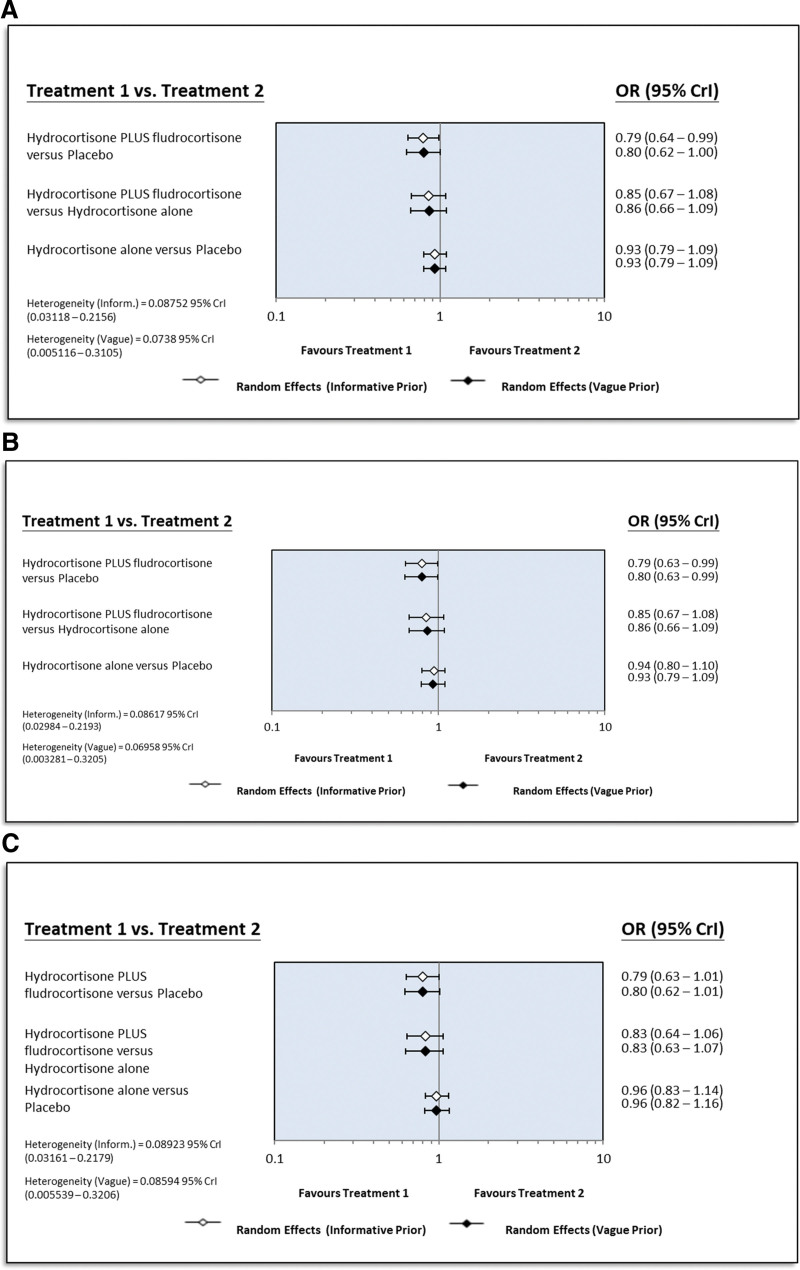
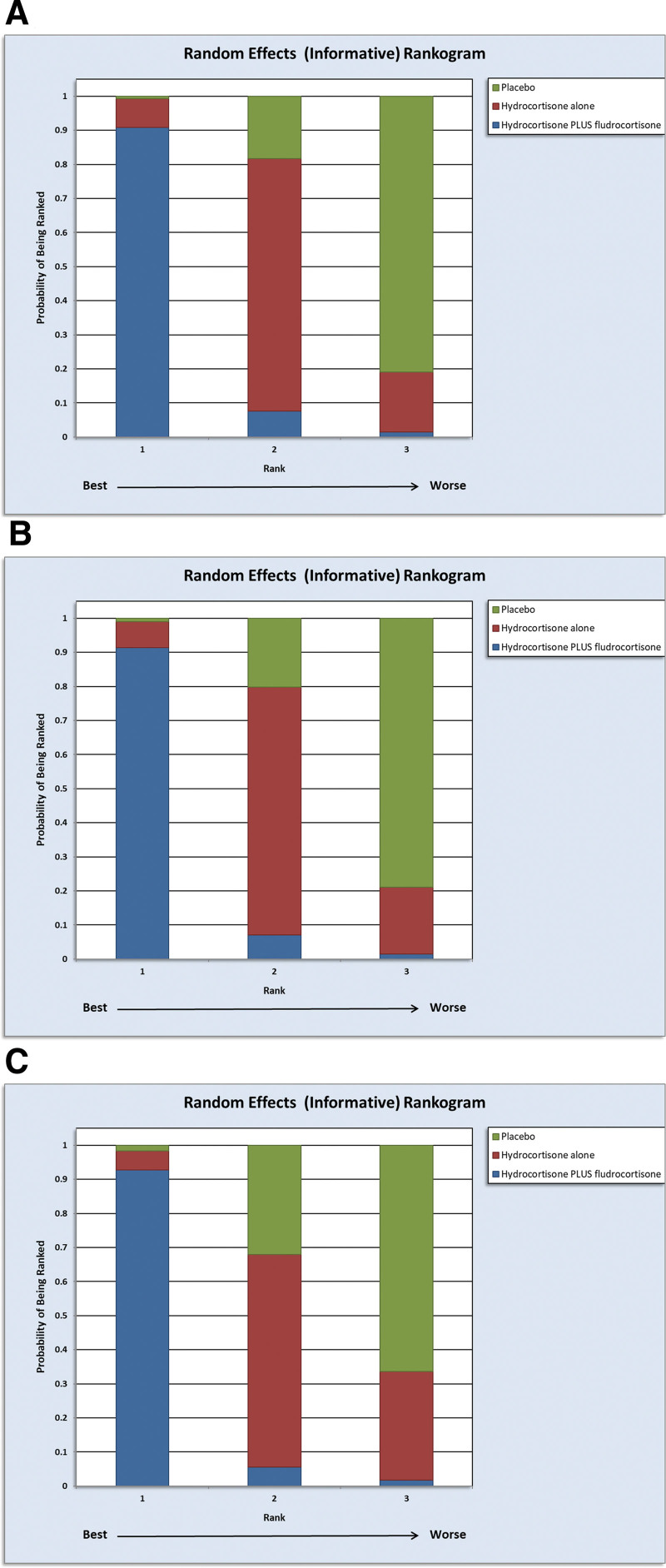
Data synthesis: A total of 19 studies involving 95,841 patients were included. Hydrocortisone plus fludrocortisone showed the lowest short-term mortality versus placebo (odds ratio [OR]: 0.79; 95% credible interval [CrI], 0.64-0.99; number needed to treat [NNT]: 21, range: 12-500; low certainty of evidence) in terms of informative priors. The surface under the cumulative ranking curve values for hydrocortisone plus fludrocortisone, hydrocortisone alone, and placebo were 0.9469, 0.4542, and 0.0989, respectively. Consistent results were observed in RCTs alone and those using a daily 200-mg dose of hydrocortisone. Although gastroduodenal bleeding or superinfection showed no clear increase, hyperglycemia risk increased. The ORs were 0.53 for placebo versus hydrocortisone plus fludrocortisone and 0.64 for placebo versus hydrocortisone alone, with very low certainty of evidence.
Conclusions: In adults with septic shock, hydrocortisone plus fludrocortisone improved short-term survival with minimal adverse events compared with hydrocortisone alone or placebo. However, these findings are not definitive due to the limited certainty of evidence and wide NNT range. Additional large-scale, placebo-controlled RCTs are needed to provide conclusive evidence.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine and Wolters Kluwer Health, Inc.
Conflict of interest statement
Dr. Huang received support for article research from the National Cheng Kung University Hospital, Tainan, Taiwan (NCKUH-11209002). The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Gotts JE, Matthay MA: Sepsis: Pathophysiology and clinical management. BMJ 2016; 353:i1585. - PubMed
-
- Fowler C, Raoof N, Pastores SM: Sepsis and adrenal insufficiency. J Intensive Care Med 2023; 38:987–996 - PubMed
-
- Evans L, Rhodes A, Alhazzani W, et al. : Surviving sepsis campaign: International Guidelines for Management of Sepsis and Septic Shock 2021. Crit Care Med 2021; 49:e1063–e1143 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
