

Outcomes of Extracorporeal Cardiopulmonary Resuscitation for In-Hospital Cardiac Arrest Among Children With Noncardiac Illness Categories
- PMID: 38156912
- PMCID: PMC11810531
- DOI: 10.1097/CCM.0000000000006153
Outcomes of Extracorporeal Cardiopulmonary Resuscitation for In-Hospital Cardiac Arrest Among Children With Noncardiac Illness Categories
Abstract
Objectives: The objective of this study was to determine the association of the use of extracorporeal cardiopulmonary resuscitation (ECPR) with survival to hospital discharge in pediatric patients with a noncardiac illness category. A secondary objective was to report on trends in ECPR usage in this population for 20 years.
Design: Retrospective multicenter cohort study.
Setting: Hospitals contributing data to the American Heart Association's Get With The Guidelines-Resuscitation registry between 2000 and 2021.
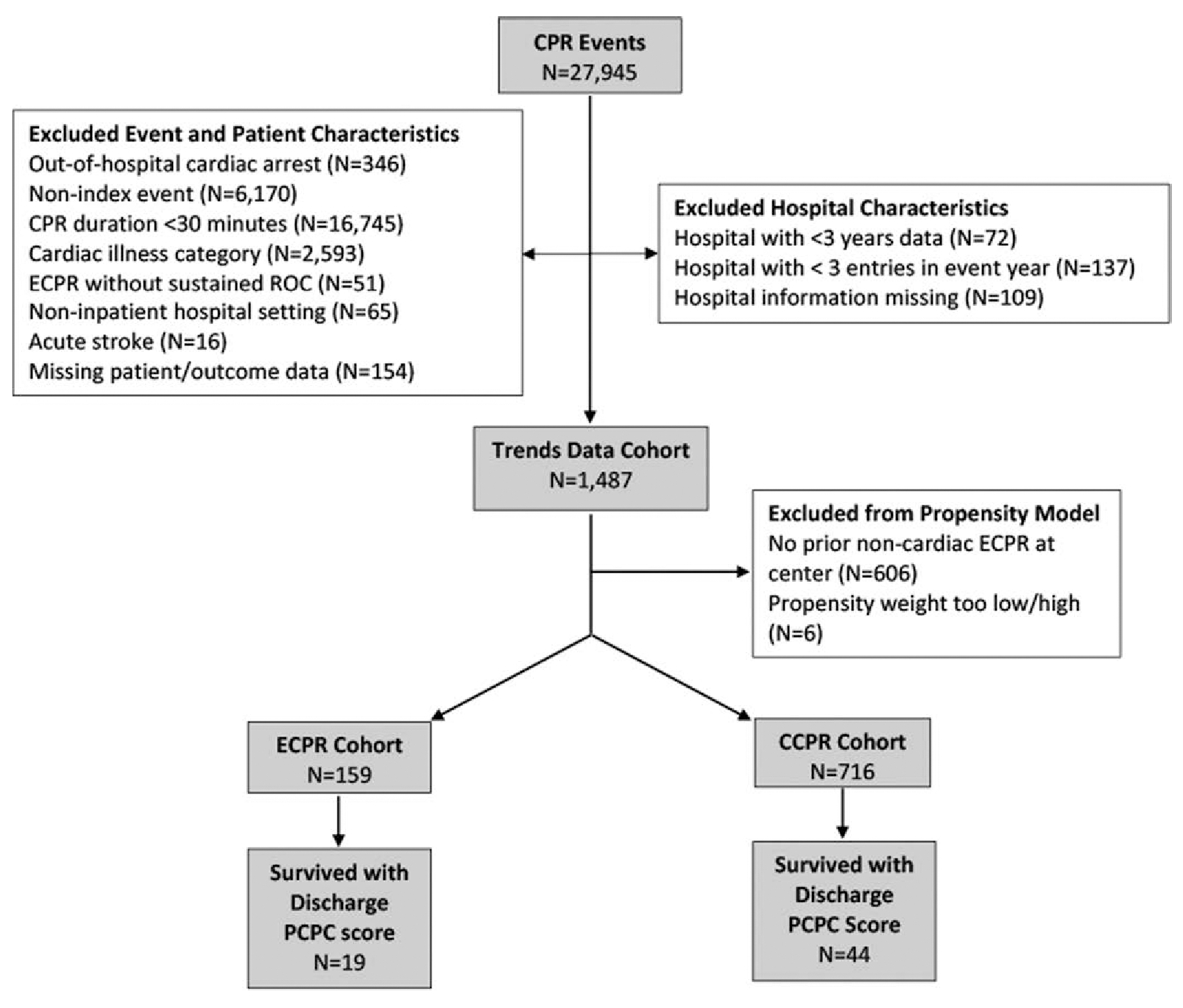
Patients: Children (<18 yr) with noncardiac illness category who received greater than or equal to 30 minutes of cardiopulmonary resuscitation (CPR) for in-hospital cardiac arrest.
Interventions: None.
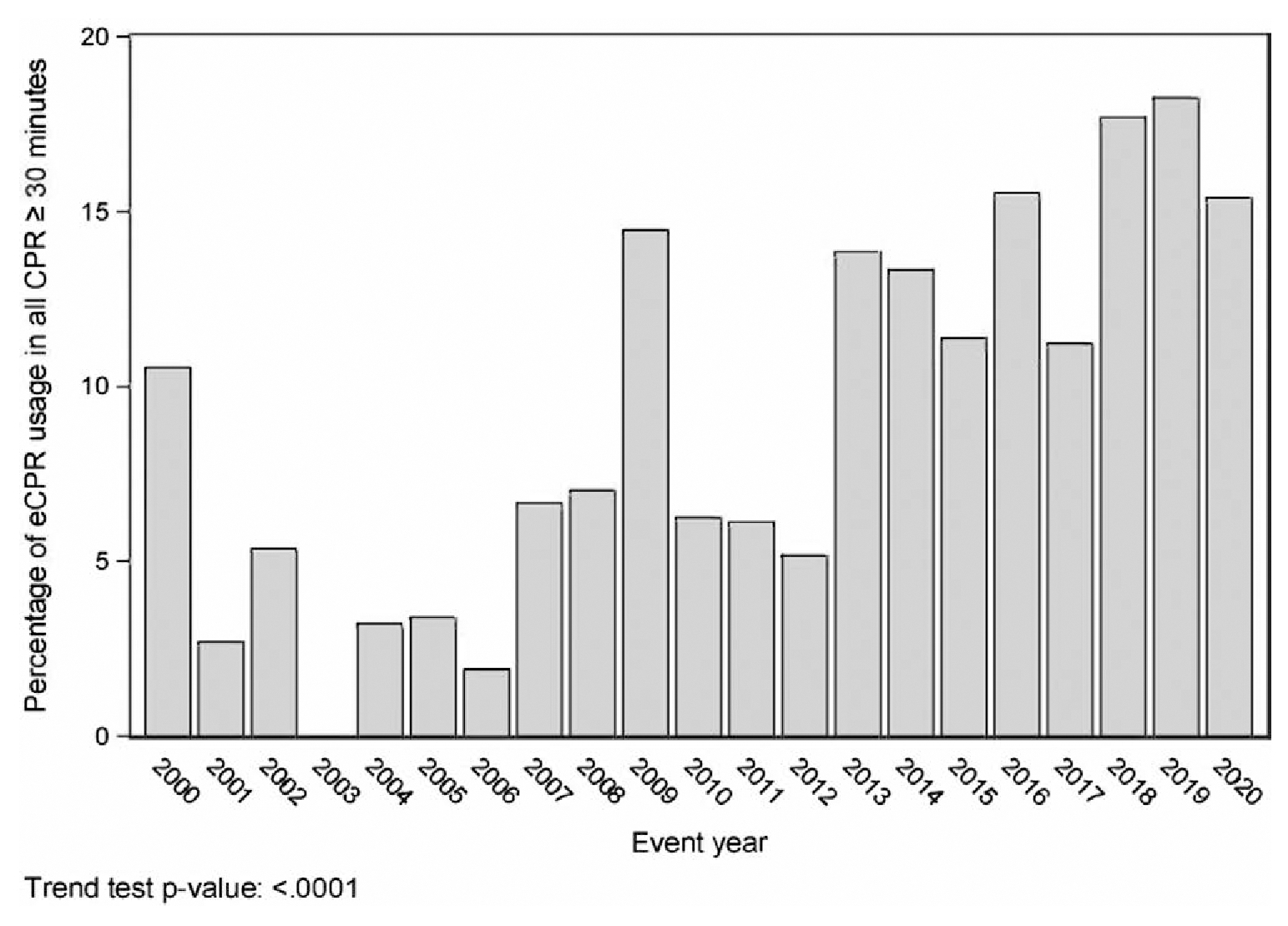
Measurements and main results: Propensity score weighting balanced ECPR and conventional CPR (CCPR) groups on hospital and patient characteristics. Multivariable logistic regression incorporating these scores tested the association of ECPR with survival to discharge. A Bayesian logistic regression model estimated the probability of a positive effect from ECPR. A secondary analysis explored temporal trends in ECPR utilization. Of 875 patients, 159 received ECPR and 716 received CCPR. The median age was 1.0 [interquartile range: 0.2-7.0] year. Most patients (597/875; 68%) had a primary diagnosis of respiratory insufficiency. Median CPR duration was 45 [35-63] minutes. ECPR use increased over time ( p < 0.001). We did not identify differences in survival to discharge between the ECPR group (21.4%) and the CCPR group (16.2%) in univariable analysis ( p = 0.13) or propensity-weighted multivariable logistic regression (adjusted odds ratio 1.42 [95% CI, 0.84-2.40; p = 0.19]). The Bayesian model estimated an 85.1% posterior probability of a positive effect of ECPR on survival to discharge.
Conclusions: ECPR usage increased substantially for the last 20 years. We failed to identify a significant association between ECPR and survival to hospital discharge, although a post hoc Bayesian analysis suggested a survival benefit (85% posterior probability).
Copyright © 2024 by the Society of Critical Care Medicine and Wolters Kluwer Health, Inc. All Rights Reserved.
Conflict of interest statement
The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Hamzah M, Othman HF, Almasri M, et al.: Survival outcomes of in-hospital cardiac arrest in pediatric patients in the USA. Eur J Pediatr 2021; 180:2513–2520 - PubMed
-
- Bembea MM, Ng DK, Rizkalla N, et al.: Outcomes after extracorporeal cardiopulmonary resuscitation of pediatric in-hospital cardiac arrest: a report from the get with the guidelines-resuscitation and the extracorporeal life support organization registries. Crit Care Med 2019; 47:e278–e285 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
