

Comparison between stapled hemorrhoidopexy and harmonic scalpel hemorrhoidectomy in the management of third- and fourth-degree piles: a randomized clinical trial
- PMID: 38157069
- PMCID: PMC11649745
- DOI: 10.1007/s00104-023-02010-9
Comparison between stapled hemorrhoidopexy and harmonic scalpel hemorrhoidectomy in the management of third- and fourth-degree piles: a randomized clinical trial
Abstract
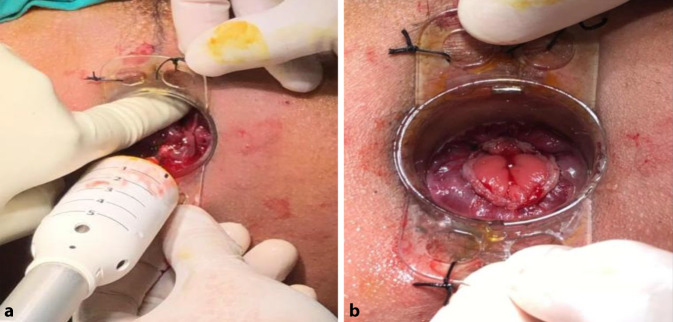
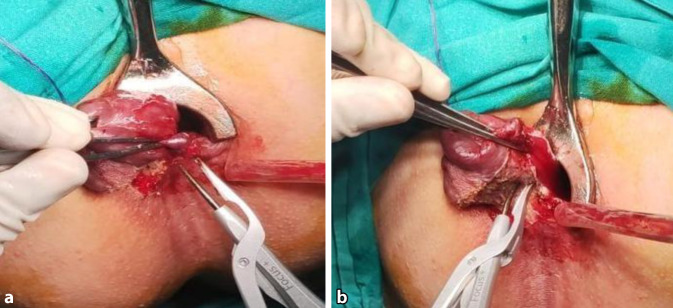
Background: This study compared the results of stapled hemorrhoidopexy (SH) and harmonic scalpel hemorrhoidectomy (HSH) in the management of grade III and grade IV piles regarding the time of the procedure, postoperative pain, patient satisfaction, wound infection, bleeding, incontinence, and recurrence within 1 year.
Patients and methods: This was a single-blind, prospective, randomized, controlled, single-center trial conducted from January to December 2022 that included 50 (68.75%) male and 20 (31.25%) female patients with third- and fourth-degree piles.
Results: The patients were divided into two groups of 35 patients each. Group I underwent SH and group II underwent HSH. The mean age of group I was 42.94 years and of group II, 42.20 years. The mean time of the procedure was 24.42 min ± 2.367 for SH and 31.48 min ± 2.21 for HSH. Postoperative pain in group I was lower than in group II during the first 2 weeks, but there was persistent mild pain in most patients in group I at the 2‑week follow-up. In group II there was significant improvement in pain after 2 weeks, with higher patient satisfaction. Wound infection was detected in 3 (5%) patients in group I and no patients in group II (p = 0.077). Postoperative bleeding occurred in 4 (11.4%) patients in group I in the form of spotting after defecation only during the first postoperative month; no bleeding was detected in group II (p = 0.039). There were 3 (15%) cases of flatus incontinence but after taking a detailed history these were found to be cases of urgency to defecate rather than incontinence. There were 7 (20%) cases of recurrence at the 1‑year follow-up in group I and 1 (2.9%) case in group II (p = 0.024).
Conclusion: Compared with SH, HSH was safer, easier, and associated with a lower incidence of recurrence after 1 year and with higher patient satisfaction.
Keywords: Bleeding; Colorectal surgery; Hemorrhoids; Prolapse; Surgical instruments.
© 2023. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: M.A. Mohamed Nada, P.B. Adly Awad, A.M. Azmy Kirollos, M. Mohamed Abdelaziz, K.M. Saad Mohamed, K. B. Adly Awad and B.H. Abdelaziz Hassan declare that they have no competing interests. Ethical approval and consent to participate: To protect patient data and privacy, all methods were carried out in accordance with relevant guidelines and regulations and all experimental protocols were approved by the Ain Shams University ethics committee with informed consent obtained from all the patients. Trial no: PACTR202310528525409, Date of Approval: 31/10/2023.
Figures






Similar articles
-
Short- and long-term results of harmonic scalpel hemorrhoidectomy versus stapler hemorrhoidopexy in treatment of hemorrhoidal disease.Asian J Surg. 2015 Oct;38(4):214-9. doi: 10.1016/j.asjsur.2014.09.004. Epub 2014 Nov 4. Asian J Surg. 2015. PMID: 25451631 Clinical Trial.
-
Randomized Controlled Trial to Compare Stapled Hemorrhoidopexy Plus Ligation Anopexy With Stapled Hemorrhoidopexy for Managing Grade III and IV Hemorrhoidal Disease.Dis Colon Rectum. 2024 Jun 1;67(6):812-819. doi: 10.1097/DCR.0000000000003273. Epub 2024 Feb 21. Dis Colon Rectum. 2024. PMID: 38380816 Clinical Trial.
-
Stapled hemorrhoidopexy vs. Harmonic Scalpel hemorrhoidectomy: a randomized trial.Dis Colon Rectum. 2005 Jun;48(6):1213-9. doi: 10.1007/s10350-004-0918-z. Dis Colon Rectum. 2005. PMID: 15793648 Clinical Trial.
-
Transanal hemorrhoidal dearterialization (THD) versus stapled hemorrhoidopexy (SH) in treatment of internal hemorrhoids: a systematic review and meta-analysis of randomized clinical trials.Int J Colorectal Dis. 2019 Jan;34(1):1-11. doi: 10.1007/s00384-018-3187-3. Epub 2018 Nov 12. Int J Colorectal Dis. 2019. PMID: 30421308
-
Meta-analysis of stapled hemorrhoidopexy vs LigaSure hemorrhoidectomy.World J Gastroenterol. 2013 Aug 7;19(29):4799-807. doi: 10.3748/wjg.v19.i29.4799. World J Gastroenterol. 2013. PMID: 23922480 Free PMC article. Review.
References
-
- Sheikh P, Régnier CH, Goron F et al (2020) The prevalence, characteristics and treatment of hemorrhoidal disease: results of an international web-based survey. J Comp Eff Res 9(17):1219–1232 - PubMed
-
- Elbatea HE, Enaba M, Elkassas G et al (2011) Indications and outcome of colonoscopy in the middle of Nile Delta of Egypt. Dig Dis Sci 56(7):2120–2123 - PubMed
-
- Gerjy R, Lindhoff-Larson A, Nyström et al (2008) Grade of prolapse and symptoms of haemorrhoids are poorly correlated: result of a classification algorithm in 270 patients. Colorectal Dis 10(7):694–700 - PubMed
-
- Goligher JC (1980) Surgery of the anus, rectum and colon. Bailliere Tindall, pp 924–925
-
- Longo A (1998) Treatment of hemorrhoids disease by reduction of mucosa and hemorrhoidal prolapse with a circular suturing device: a new procedure. In 6th Warld Congress of Endoscopic Surgery
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical