

Genetic and transcriptomic analyses of diffuse large B-cell lymphoma patients with poor outcomes within two years of diagnosis
- PMID: 38158444
- PMCID: PMC10912034
- DOI: 10.1038/s41375-023-02120-7
Genetic and transcriptomic analyses of diffuse large B-cell lymphoma patients with poor outcomes within two years of diagnosis
Abstract
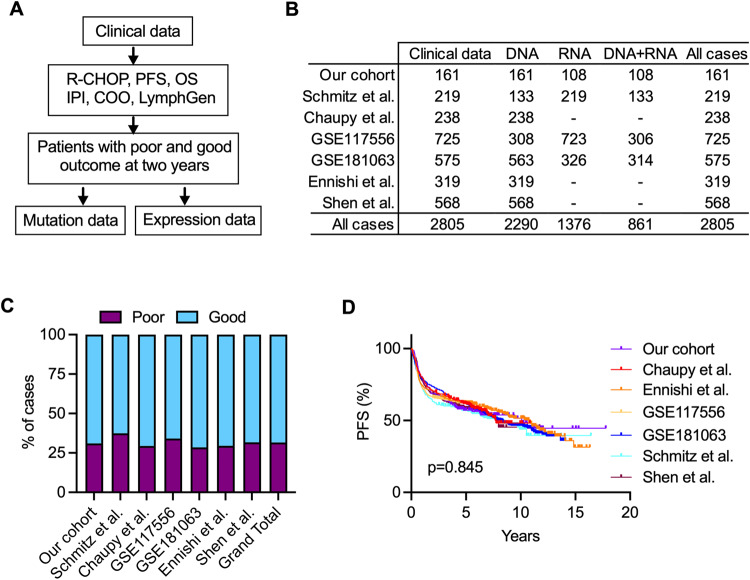
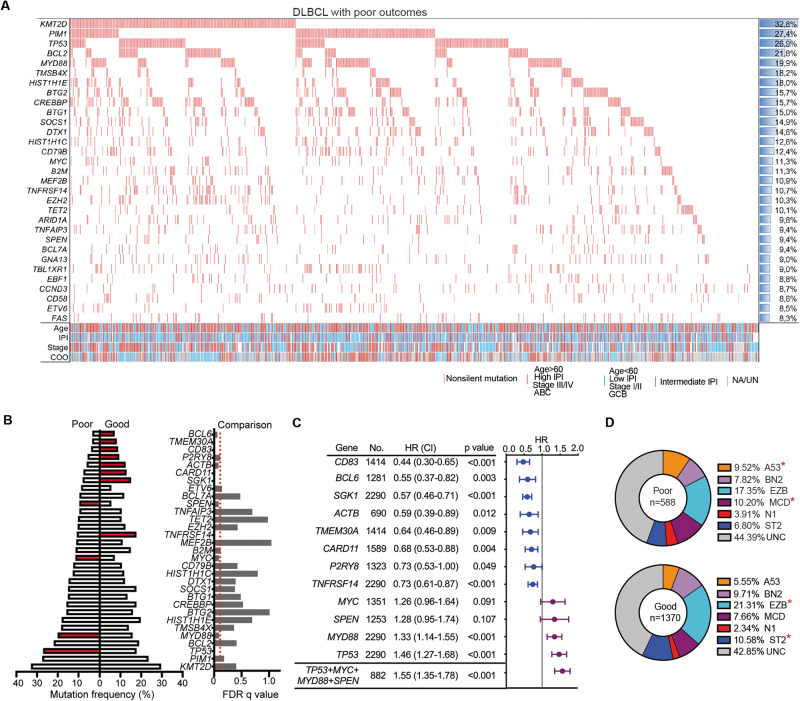
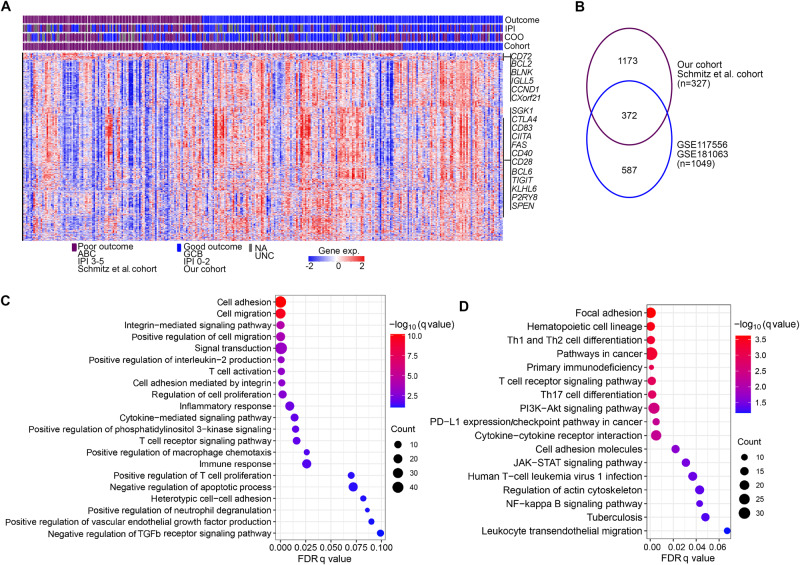
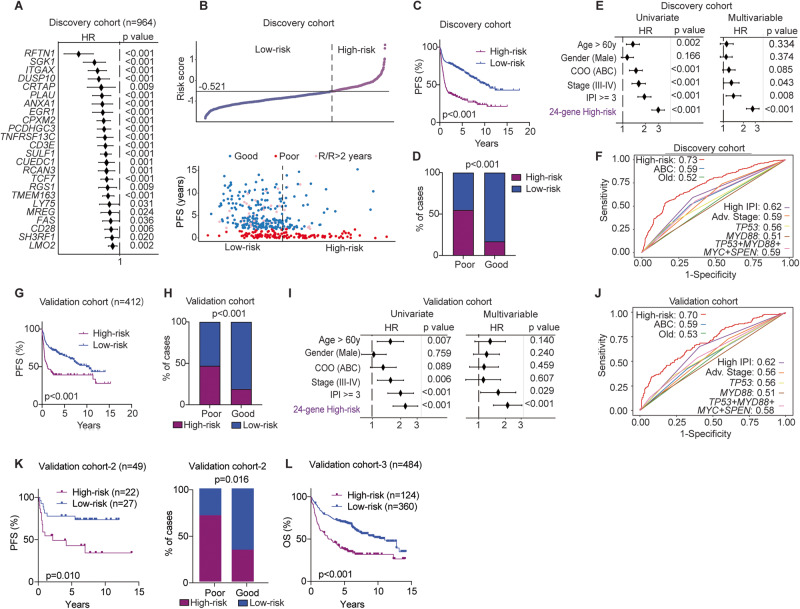
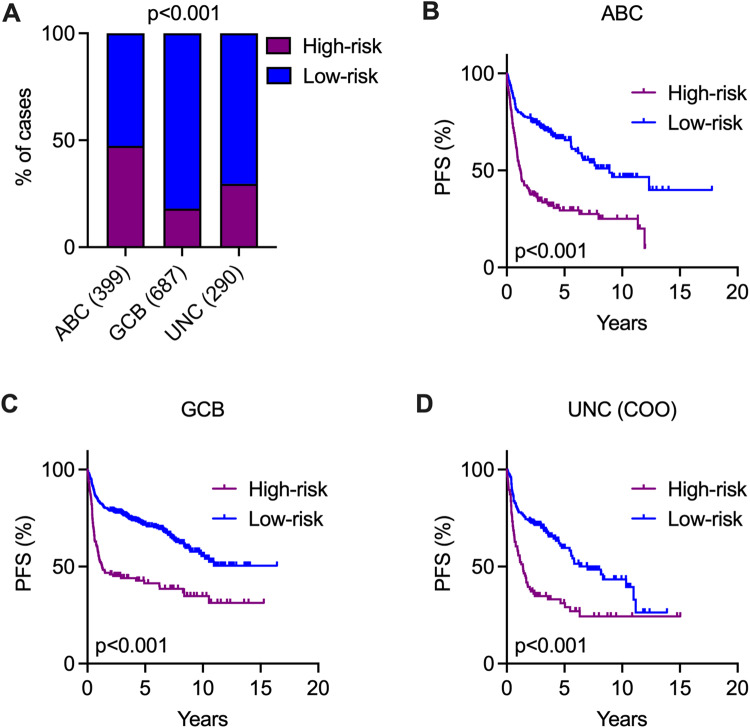
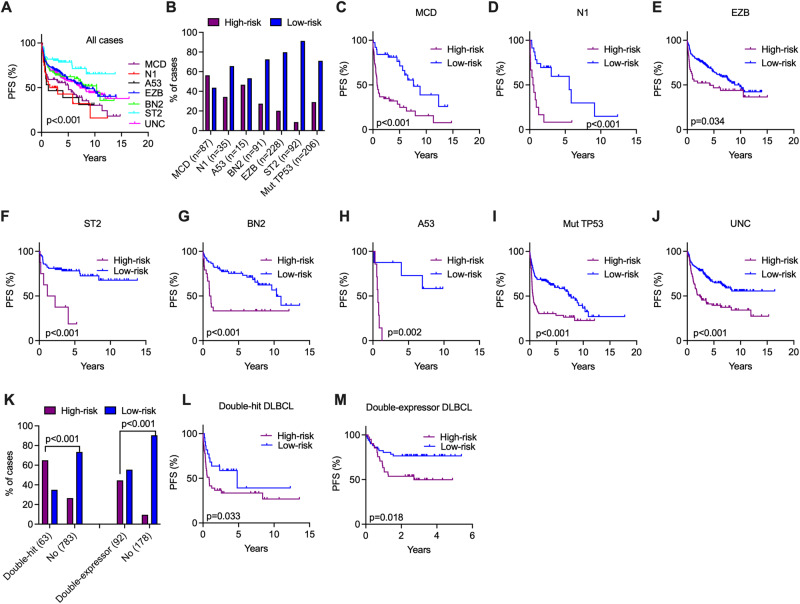
Despite the improvements in clinical outcomes for DLBCL, a significant proportion of patients still face challenges with refractory/relapsed (R/R) disease after receiving first-line R-CHOP treatment. To further elucidate the underlying mechanism of R/R disease and to develop methods for identifying patients at risk of early disease progression, we integrated clinical, genetic and transcriptomic data derived from 2805 R-CHOP-treated patients from seven independent cohorts. Among these, 887 patients exhibited R/R disease within two years (poor outcome), and 1918 patients remained in remission at two years (good outcome). Our analysis identified four preferentially mutated genes (TP53, MYD88, SPEN, MYC) in the untreated (diagnostic) tumor samples from patients with poor outcomes. Furthermore, transcriptomic analysis revealed a distinct gene expression pattern linked to poor outcomes, affecting pathways involved in cell adhesion/migration, T-cell activation/regulation, PI3K, and NF-κB signaling. Moreover, we developed and validated a 24-gene expression score as an independent prognostic predictor for treatment outcomes. This score also demonstrated efficacy in further stratifying high-risk patients when integrated with existing genetic or cell-of-origin subtypes, including the unclassified cases in these models. Finally, based on these findings, we developed an online analysis tool ( https://lymphprog.serve.scilifelab.se/app/lymphprog ) that can be used for prognostic prediction for DLBCL patients.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Coiffier B, Lepage E, Briere J, Herbrecht R, Tilly H, Bouabdallah R, et al. CHOP chemotherapy plus rituximab compared with CHOP alone in elderly patients with diffuse large-B-cell lymphoma. N Engl J Med. 2002;346:235–42. - PubMed
-
- Sarkozy C, Coiffier B. Primary refractory diffuse large B cell lymphoma in the rituximab era. Curr Opin Oncol. 2015;27:377–83. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
