

Biochemical progression free and overall survival among Black men with stage IV prostate cancer in South Africa: Results from a prospective cohort study
- PMID: 38158645
- PMCID: PMC10807684
- DOI: 10.1002/cam4.6739
Biochemical progression free and overall survival among Black men with stage IV prostate cancer in South Africa: Results from a prospective cohort study
Abstract
Background: Men of African descent are disproportionately affected by prostate cancer (PCa), and many have metastatic disease at presentation. In South Africa (SA), androgen deprivation therapy (ADT) is the first-line treatment for stage IV PCa.
Objective: To identify predictors of overall survival (OS) in Black South African men with stage IV PCa treated with ADT.
Design, setting, and participants: Men diagnosed with prostate cancer (3/22/2016-10/30/2020) at Chris Hani Baragwanath Academic Hospital in Soweto, Johannesburg, were recruited for the Men of African Descent with Cancer of the Prostate study. We included men with newly diagnosed stage IV PCa treated with ADT who had a prostate-specific antigen (PSA) level drawn prior to initiation of ADT and had ≥1 PSA drawn ≥12 weeks after ADT start.
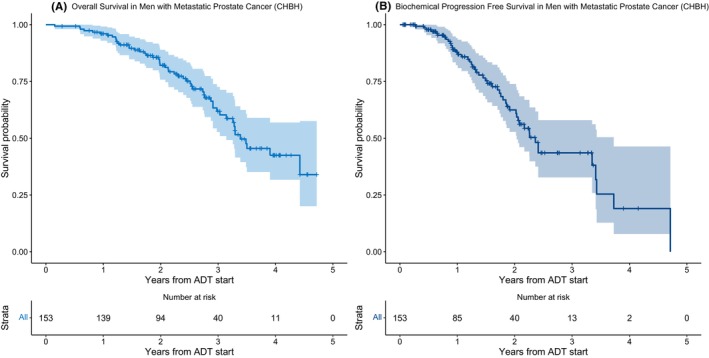
Outcomes measures and statistical analysis: We used Kaplan-Meier statistics to estimate OS and Cox regression models to identify predictors of OS.
Results and limitations: Of the 1097 men diagnosed with prostate cancer, we included 153 men with stage IV PCa who received ADT and met PSA requirements. The median age was 68.0 years (interquartile range 64-73 years). Median OS from time of ADT initiation was 3.39 years (95% confidence interval (CI): 3.14%-noncalculable), while biochemical progression-free survival was 2.36 years (95% CI: 2.03%-3.73%). Biochemical progression (HR 3.52, 95% CI: 1.85%-6.70%), PSA nadir level >4 ng/mL (HR 3.77, 95% CI: 1.86%-7.62%), alkaline phosphatase level at diagnosis >150 IU/dL (HR 3.09, 95% CI: 1.64%-5.83%), and hemoglobin at diagnosis <13.5 g/dL (HR 2.90, 95% CI: 1.28%-6.56%) were associated with worse OS.
Conclusions: In this study, we identified factors associated with poor OS among Black South African men with stage IV PCa treated with ADT. These factors may be useful in identifying patients for upfront treatment escalation, including the use of docetaxel chemotherapy or escalation of therapy at the time of biochemical progression.
Patient summary: In this study, we found that high alkaline phosphatase level, anemia at diagnosis, and high PSA nadir after initiation of androgen deprivation therapy are associated with worse overall survival among Black South African men treated with androgen deprivation therapy for metastatic prostate cancer.
Keywords: cancer management; hormone therapy; metastasis; prostate cancer.
© 2023 The Authors. Cancer Medicine published by John Wiley & Sons Ltd.
Conflict of interest statement
Alfred Neugut: Otsuka, United Biosource Corp, Hospira, Eisai, and GlaxoSmithKline (Consulting/advisory relationship); EHE Intl (Scientific Advisory Board); Otsuka (Research Funding); Yoanna Pumpalova: Pfizer (Ownership Interest). The other authors indicated no financial relationships.
Figures
References
-
- Tindall EA, Bornman MSR, van Zyl S, et al. Addressing the contribution of previously described genetic and epidemiological risk factors associated with increased prostate cancer risk and aggressive disease within men from South Africa. BMC Urol. 2013;13:74. doi:10.1186/1471-2490-13-74 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
