

Homelessness and Emergency Department Use: Wait Time Disparities Across Triage Acuity Levels
- PMID: 38161888
- PMCID: PMC10756006
- DOI: 10.7759/cureus.49520
Homelessness and Emergency Department Use: Wait Time Disparities Across Triage Acuity Levels
Abstract
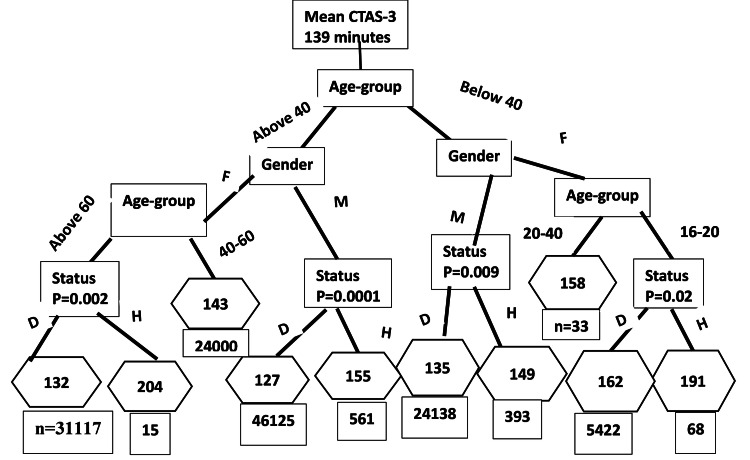
Introduction Certain patient groups perceive specific barriers to accessing primary care, resulting in increased emergency department (ED) use for non-emergency conditions. There is evidence coming from other countries that homeless people are treated differently in accessing emergency services. Examination of ED wait time by demographic characteristics provides pertinent information to identify subgroups that are more subject to the consequences or causes of access block and delayed treatment. Methods We analyzed five years of Emergency Department Information System (EDIS) visit records of the largest tertiary care center in Atlantic Canada. The wait time from triage to seeing a physician was the outcome, housing status was the main exposure, and age and gender were the predictors. Quantile regressions were carried out to identify the influence of homeless visits in meeting the Canadian Association of Emergency Physicians (CAEP) wait time benchmarks for each Canadian Triage and Acuity Scale (CTAS) level. The classification and regression tree method was used to quantify and classify the demographic subgroups contributing to wait time disparities across CTAS levels. Results Homeless visit median wait times that exceeded the three-hour CAEP benchmark were significantly longer for urgent (by 40 minutes, CI: 25-55), semi-urgent (by 31 minutes, CI: 17-45), and non-urgent (by 57 minutes, CI: 25-89) than acuity level-matched domiciled visit wait times. At the 50th percentile, one-hour benchmark homeless triaged as semi-urgent waited (median=20 minutes, CI: 12-28) longer, and no other triage-level differences were found at this benchmark. Homeless emergent-level visits that exceeded the three-hour benchmark were 28 minutes, on average, shorter than domiciled patients of the same acuity level. Homeless females above 40 stayed the longest for non-urgent care (mean=173 minutes), 82 minutes longer (p=0.0001) than age-gender-acuity level-matched domiciled patients. Homelessness was the most prominent ED wait time classifier for non-urgent, ED visits. Overall, homeless patients triaged as CTAS-5 waited 30 minutes longer (p=0.0001) than domiciled patients triaged as CTAS-5. Homeless male 16-20-year-olds waited the shortest time of 72 minutes. Conclusion Homelessness-related wait time disparities exist in the low acuity non-urgent-level ED visits more than in the other levels, supporting the theory that lack of primary care access is a driver of ED use in this group. Our acuity level analysis supports that homeless people of a certain age (older) and gender groups (female) wait longer than their age-gender-matched domiciled patients to be seen by a physician in low acuity level presentations. Given the pattern of the homeless being seen earlier or statistically similar in emergent-level visits compared to matched domiciled patients and that 16-20-year-old homeless males were seen on average within 72 minutes (the shortest mean wait time reported for the triage level CTAS-5), we decline the notion of discrimination at the study site ED. If homeless patients' non-urgent needs were met elsewhere, pressure on the ED to meet benchmarks might be reduced.
Keywords: canadian triage acuity scale-based ed visits; disparities across demographic subgroups; homelessness; wait time; wait time benchmarks.
Copyright © 2023, Weerasinghe et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures




Similar articles
-
Identifying Acuity Level-Based Adult Emergency Department Use Time Trends Across Demographic Characteristics.Cureus. 2021 Feb 8;13(2):e13225. doi: 10.7759/cureus.13225. Cureus. 2021. PMID: 33728175 Free PMC article.
-
Are wait times and length of stay in Alberta emergency departments for children's mental health meeting national benchmarks? Trends from 2002 to 2008.Paediatr Child Health. 2013 Jun;18(6):e26-31. Paediatr Child Health. 2013. PMID: 24421704 Free PMC article.
-
A determination of emergency department pre-triage times in patients not arriving by ambulance compared to widely used guideline recommendations.CJEM. 2017 Jul;19(4):265-270. doi: 10.1017/cem.2016.398. Epub 2016 Dec 5. CJEM. 2017. PMID: 27917744
-
About time! A scoping review of public-facing emergency department wait time displays in Canada.CJEM. 2022 Aug;24(5):503-508. doi: 10.1007/s43678-022-00301-4. Epub 2022 Apr 28. CJEM. 2022. PMID: 35482228
-
Emergency department wait times in concordance with blood alcohol content and subsequent alcohol use disorder.J Osteopath Med. 2025 Apr 25. doi: 10.1515/jom-2024-0168. Online ahead of print. J Osteopath Med. 2025. PMID: 40270462 Review.
Cited by
-
Geriatric Population Triage: The Risk of Real-Life Over- and Under-Triage in an Overcrowded ED: 4- and 5-Level Triage Systems Compared: The CREONTE (Crowding and R E Organization National TriagE) Study.J Pers Med. 2024 Feb 9;14(2):195. doi: 10.3390/jpm14020195. J Pers Med. 2024. PMID: 38392628 Free PMC article.
References
-
- Hospital Emergency Care & Homelessness. [ Mar; 2023 ]. 2017. https://www.homelesshub.ca/blog/hospital-emergency-care-homelessness https://www.homelesshub.ca/blog/hospital-emergency-care-homelessness
-
- Use of point of care sonography by emergency physicians. J Henneberry R, Hanson A, Healey A, et al. CJEM. 2012;14:106–112. - PubMed
-
- Myths versus facts in emergency department overcrowding and hospital access block. Richardson DB, Mountain D. Med J Aust. 2009;190:369–374. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous