

Downhill Varices and Apical Lung Cancer Without Superior Vena Cava Syndrome
- PMID: 38162006
- PMCID: PMC10754591
- DOI: 10.14309/crj.0000000000001236
Downhill Varices and Apical Lung Cancer Without Superior Vena Cava Syndrome
Abstract
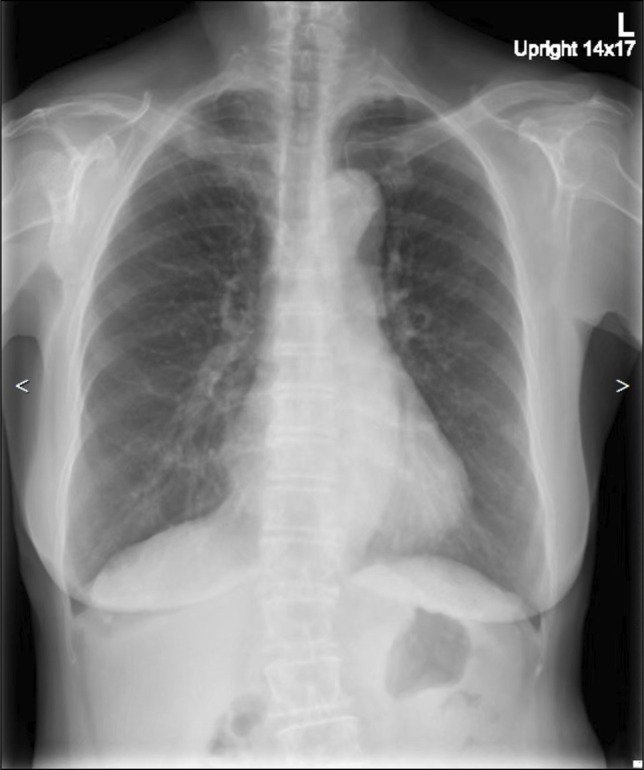
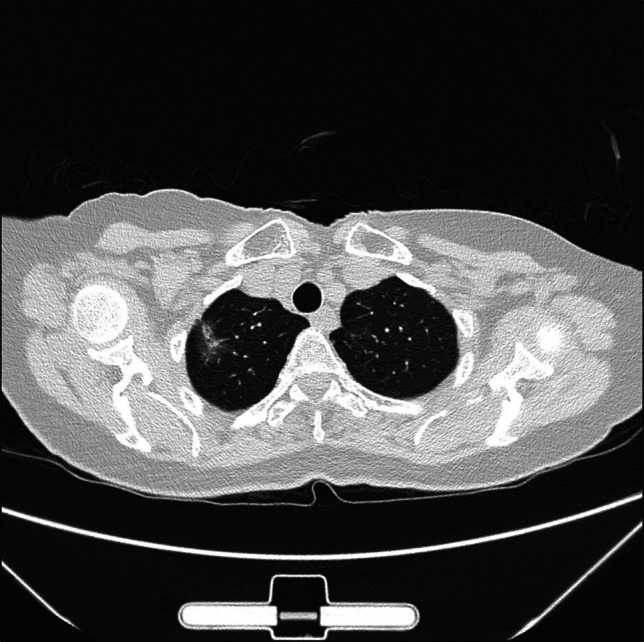
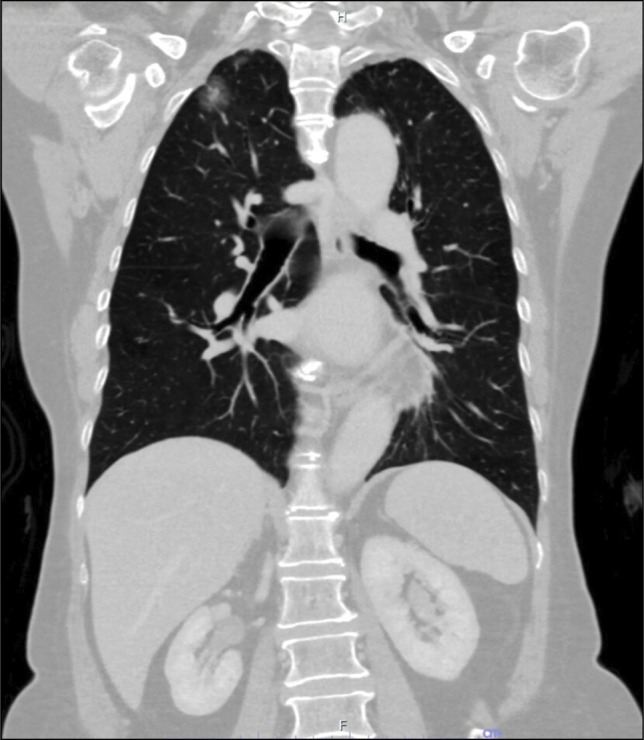
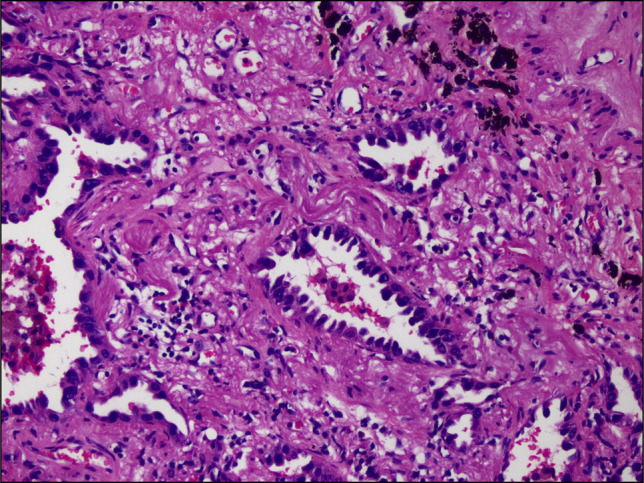
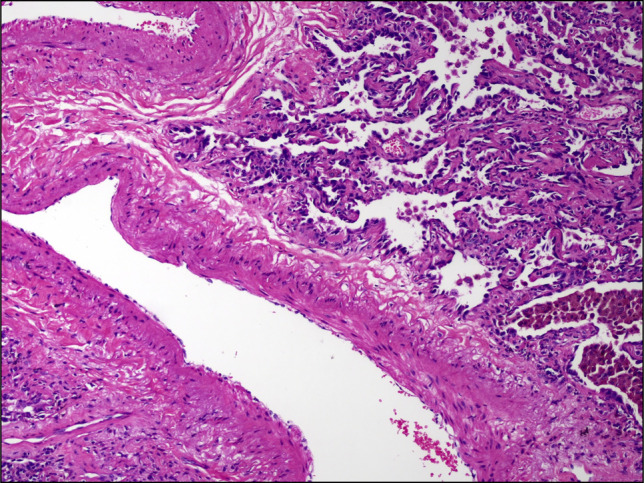
A 75-year-old woman with hypertension, dyslipidemia, thalassemia trait, osteoarthritis of the knees, and hyperthyroidism presented with bloating, abdominal discomfort, and change in stool caliber underwent an esophagogastroduodenoscopy. The esophagogastroduodenoscopy revealed varices at the middle of esophagus, which were diagnosed to be downhill esophageal varices (DEVs). DEVs occur mainly from the superior vena cava (SVC) obstruction; however, in the absence of obstruction, angiogenesis and thrombosis could be the etiology. In our patient, computed tomography showed a pulmonary nodule located at periphery of the right upper lung without SVC contact nor obstruction. The nodule was later proven to be an adenocarcinoma. Thus, our patient showed the possibility that adenocarcinoma of the lung might associated with the DEV through a mechanism other than SVC obstruction. Recognition and differentiation of DEV from other benign venous blebs of the esophagus are important, and once detected, further investigation with computed tomography of the chest is recommended.
Keywords: SVC obstruction; SVC syndrome; downhill varices; esophageal varices; lung cancer; varix.
© 2023 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of The American College of Gastroenterology.
Figures

References
-
- Israelski M, Simchowitz H. 1. Roentgendiagnostic der esophagus varizen. Laryngol Rhinol Otol. 1932;22:208–18.
-
- Ali H, Pamarthy R, Bolick NL, Ali E, Paleti S, Kapuria D. Downhill esophageal varices: A systematic review of the case reports. Explor Med. 2022;3(4):317–30.
-
- Savoy AD, Wolfsen HC, Paz-Fumagalli R, Raimondo M. Endoscopic therapy for bleeding proximal esophageal varices: A case report. Gastrointest Endosc. 2004;59(2):310–3. - PubMed
-
- Tanaka H, Nakahara K, Goto K. Two cases of downhill esophageal varices associated with superior vena cava syndrome due to lung cancer [in Japanese]. Nihon Kyobu Shikkan Gakkai Zasshi. 1991;29(11):1484–8. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
