

Rapid Arterial Occlusion Evaluation (RACE) Tool in Detecting Large Cerebral Vessel Occlusions; a Systematic Review and Meta-Analysis
- PMID: 38162382
- PMCID: PMC10757574
- DOI: 10.22037/aaem.v12i1.2152
Rapid Arterial Occlusion Evaluation (RACE) Tool in Detecting Large Cerebral Vessel Occlusions; a Systematic Review and Meta-Analysis
Abstract
Introduction: Large vessel occlusion (LVO) strokes are linked to higher mortality rates and a greater risk of long-term disability. This study aimed to evaluate the diagnostic performance of the Rapid Arterial Occlusion Evaluation (RACE) tool in detecting LVO through a systematic review and meta-analysis.
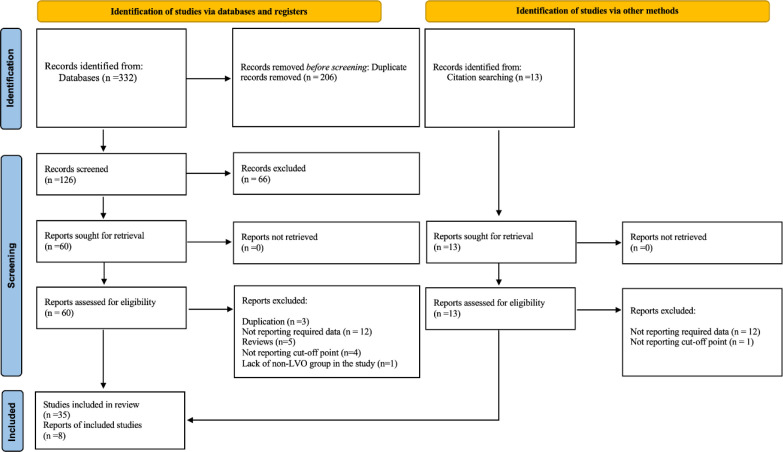
Methods: A comprehensive search was conducted across online databases including PubMed, Embase, Scopus, and Web of Science, up to June 25th, 2023. Additionally, a manual search on Google and Google Scholar was performed to identify studies that assessed the diagnostic accuracy of the RACE scale in detecting LVO among patients with stroke symptoms.
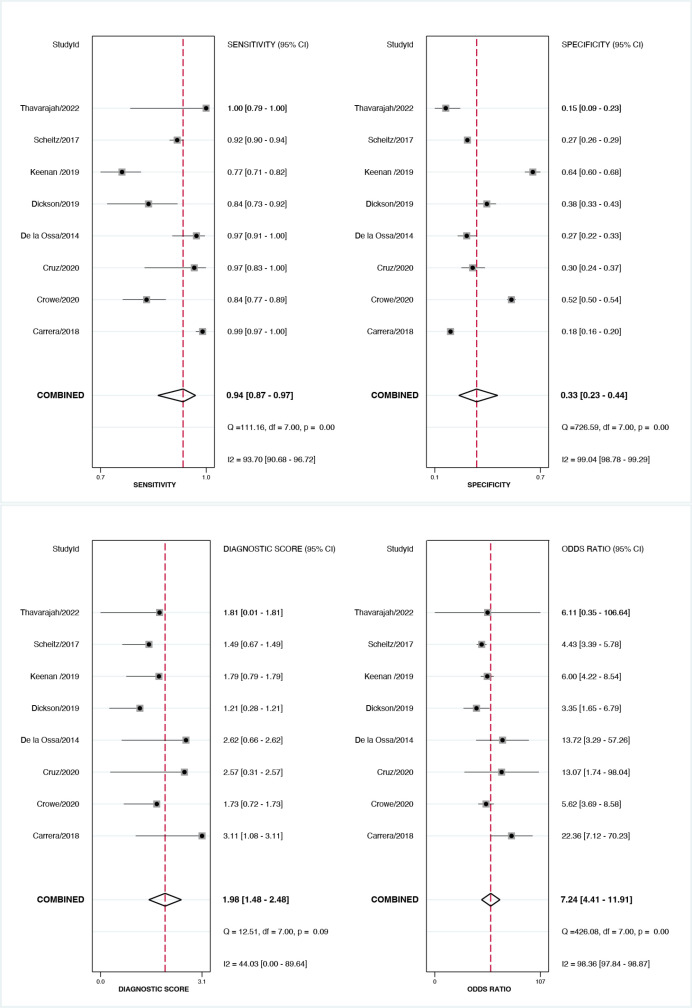
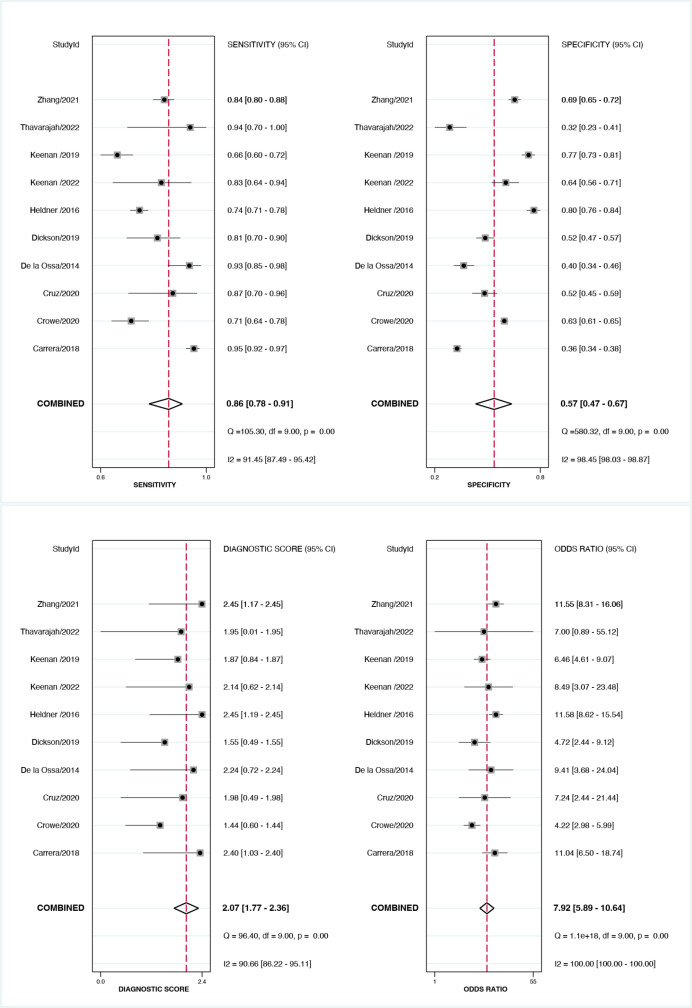
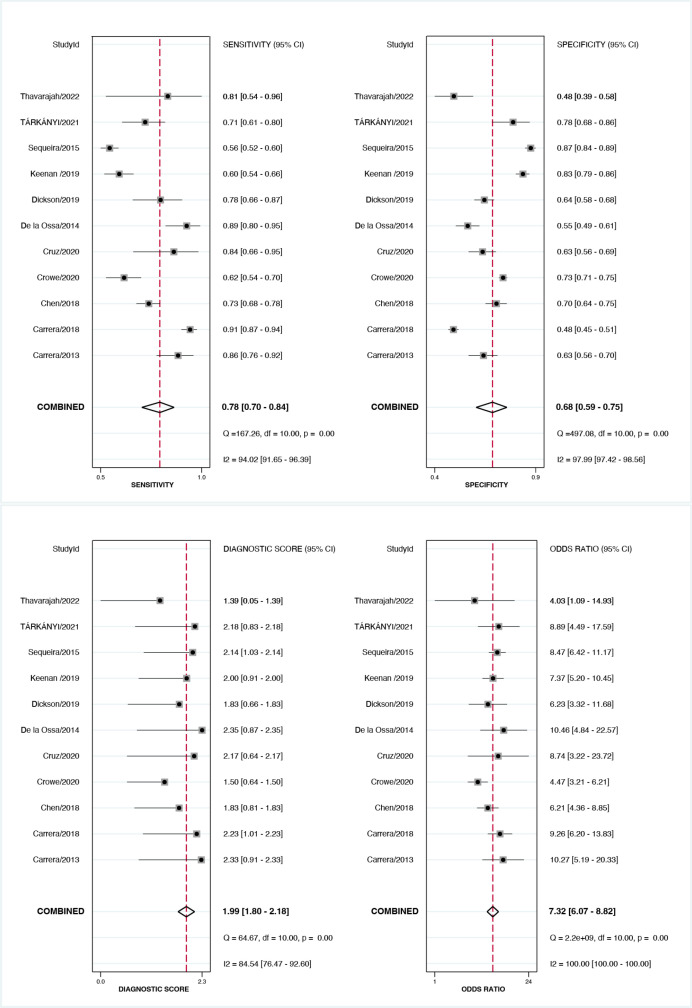
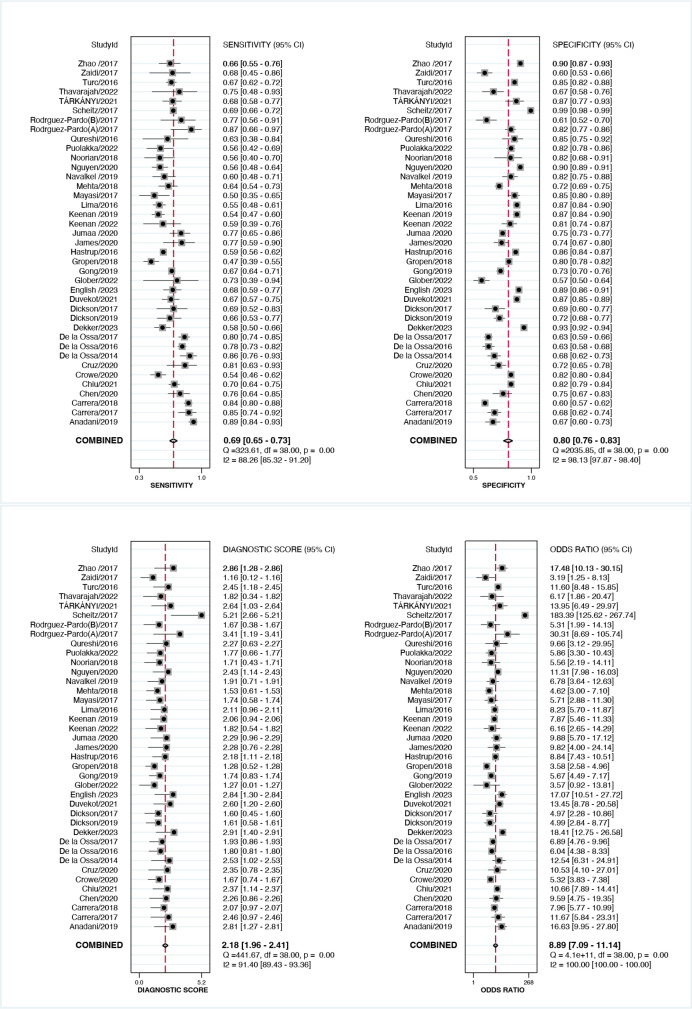
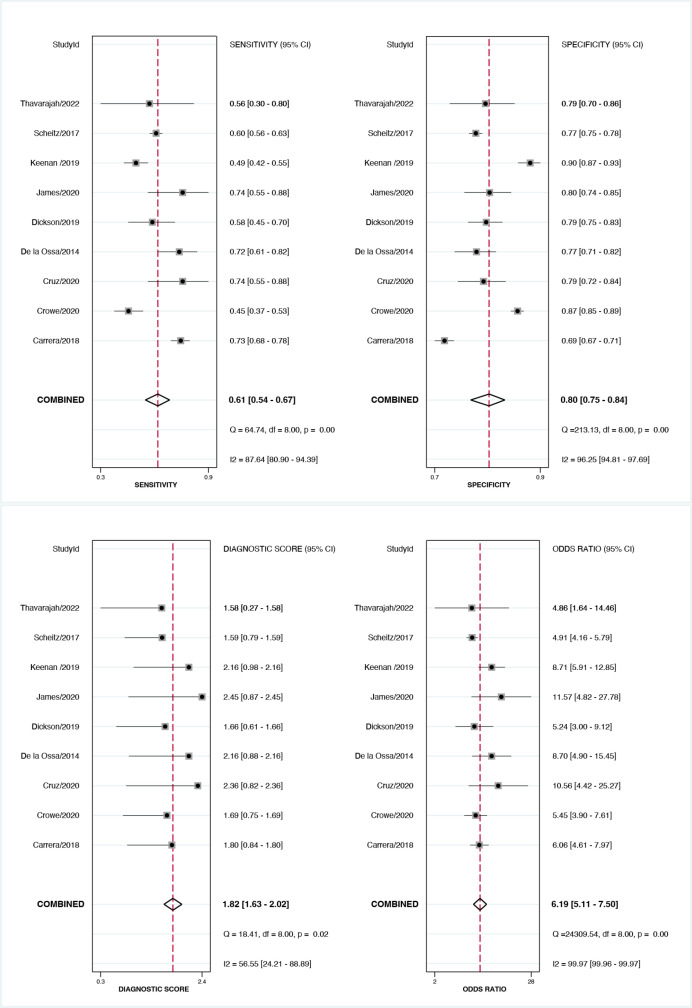
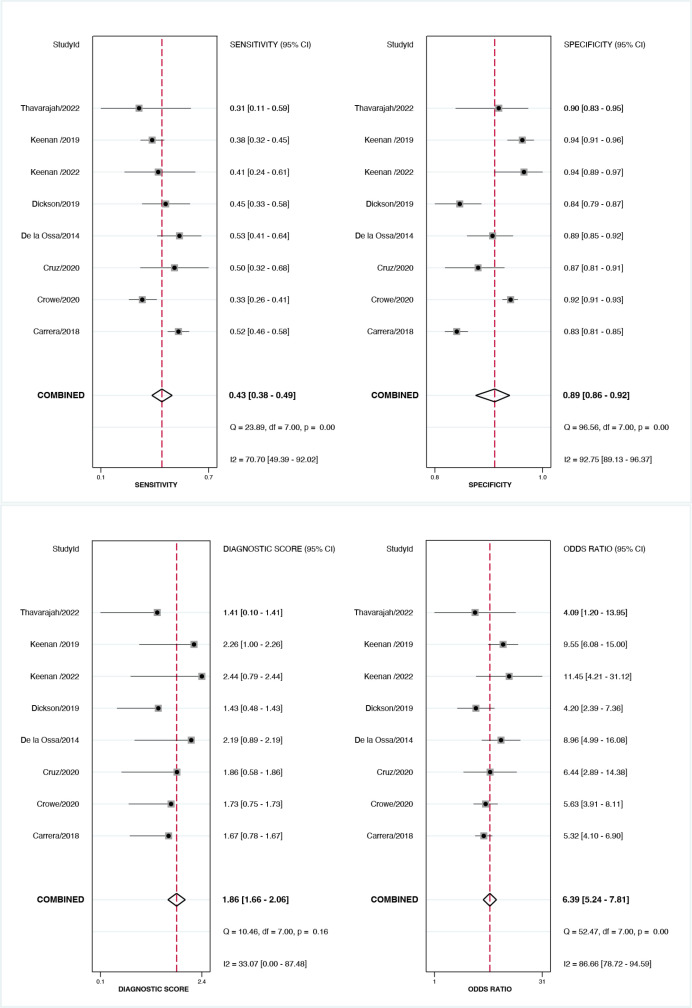
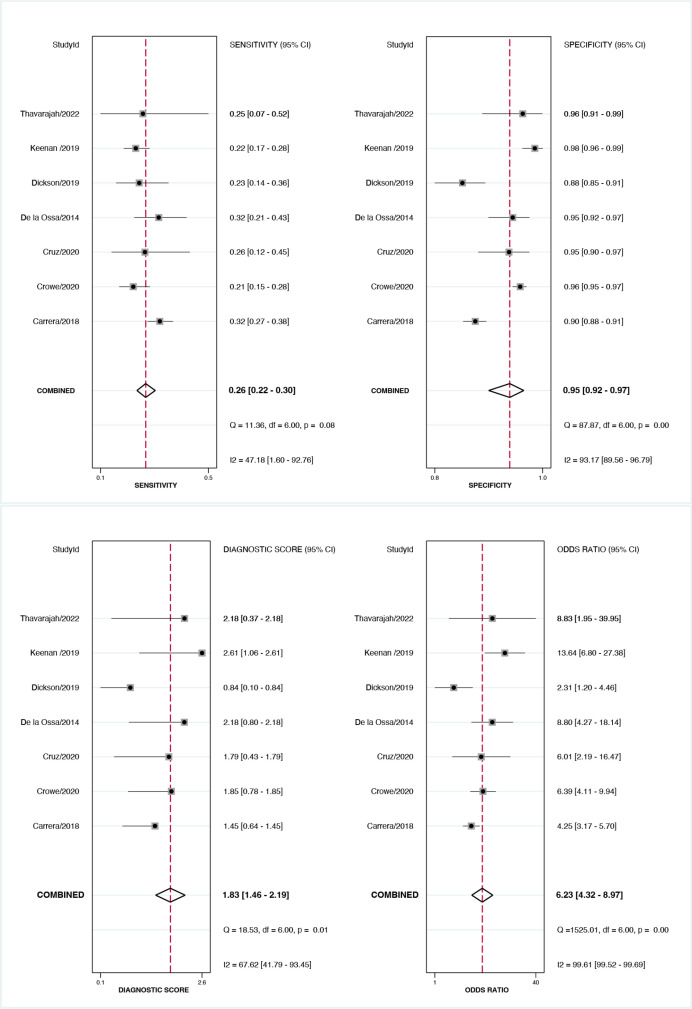
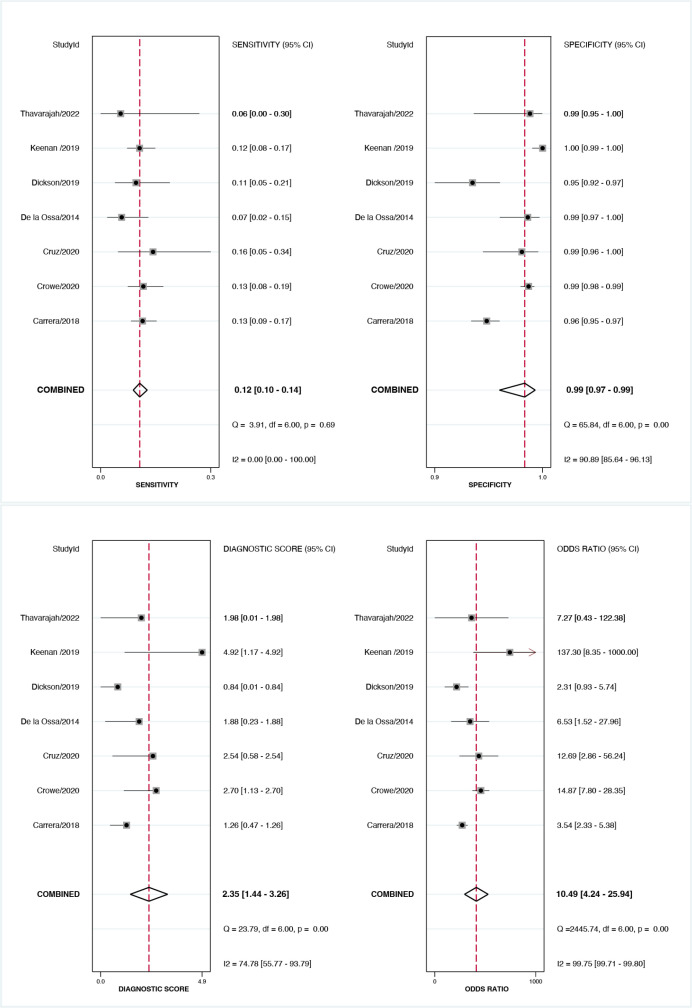
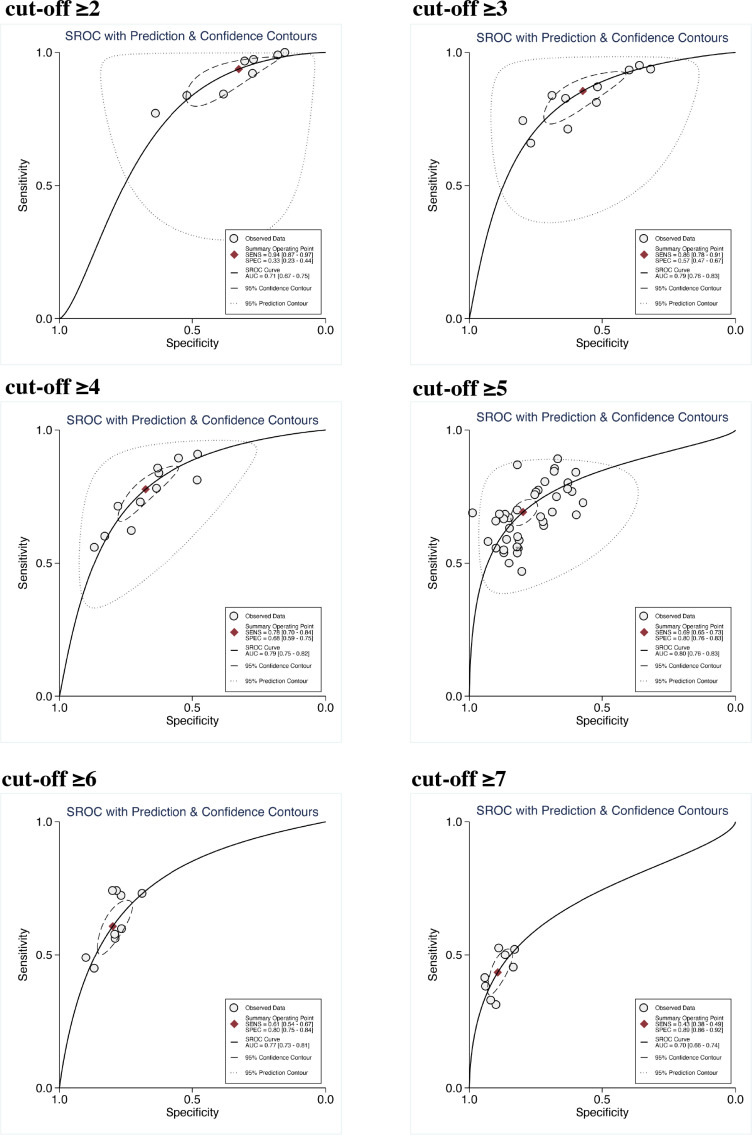
Results: Data extracted from 43 studies were analyzed. The optimal cut-off points were determined to be 3 and 4, with a sensitivity of 0.86 (95% confidence interval (CI): 0.78, 0.91) and specificity of 0.57 (95% CI: 0.49, 0.67) for cut-off ≥3, and a sensitivity of 0.78 (95% CI: 0.70, 0.84) and specificity of 0.68 (95% CI: 0.59, 0.75) for cut-off ≥4. Subgroup meta-regression analysis revealed significant variations in sensitivity and specificity. RACE scale's sensitivity was significantly higher in LVO detection in suspected stroke cases, in pre-hospital settings, prospective design studies, and when considering both anterior and posterior occlusions for LVO definition. RACE scale's specificity was significantly higher when evaluating confirmed stroke cases, in-hospital settings, and considering only anterior occlusions for LVO definition and retrospective design studies. Notably, RACE exhibited higher sensitivity and specificity when utilized by neurologists and physicians compared to other emergency staff. Despite these variations, our study found comparable diagnostic accuracy across different conditions.
Conclusion: A high level of evidence indicates that the RACE scale lacks promising diagnostic value for detection of LVOs. A sensitivity range of 0.69 to 0.86 is insufficient for a screening tool intended to aid in the diagnosis of strokes, considering the substantial morbidity and mortality associated with this condition.
Keywords: Arterial occlusive diseases; Clinical decision rules; Diagnosis; Meta-analysis; Systematic review.
Conflict of interest statement
None
Figures
Similar articles
-
Cincinnati Prehospital Stroke Scale (CPSS) as a Screening Tool for Early Identification of Cerebral Large Vessel Occlusions; a Systematic Review and Meta-analysis.Arch Acad Emerg Med. 2024 Mar 26;12(1):e38. doi: 10.22037/aaem.v12i1.2242. eCollection 2024. Arch Acad Emerg Med. 2024. PMID: 38737135 Free PMC article. Review.
-
Performance of the RACE Score for the Prehospital Identification of Large Vessel Occlusion Stroke in a Suburban/Rural EMS Service.Prehosp Emerg Care. 2019 Sep-Oct;23(5):612-618. doi: 10.1080/10903127.2019.1573281. Epub 2019 Feb 20. Prehosp Emerg Care. 2019. PMID: 30668202
-
Design and validation of a prehospital stroke scale to predict large arterial occlusion: the rapid arterial occlusion evaluation scale.Stroke. 2014 Jan;45(1):87-91. doi: 10.1161/STROKEAHA.113.003071. Epub 2013 Nov 26. Stroke. 2014. PMID: 24281224
-
Recognition of Stroke in the Emergency Room (ROSIER) Scale in Identifying Strokes and Transient Ischemic Attacks (TIAs); a Systematic Review and Meta-Analysis.Arch Acad Emerg Med. 2023 Oct 5;11(1):e67. doi: 10.22037/aaem.v11i1.2135. eCollection 2023. Arch Acad Emerg Med. 2023. PMID: 37840869 Free PMC article. Review.
-
Field Assessment Stroke Triage for Emergency Destination: A Simple and Accurate Prehospital Scale to Detect Large Vessel Occlusion Strokes.Stroke. 2016 Aug;47(8):1997-2002. doi: 10.1161/STROKEAHA.116.013301. Epub 2016 Jun 30. Stroke. 2016. PMID: 27364531 Free PMC article.
Cited by
-
Enhancing Stroke Recognition: A Comparative Analysis of Balance and Eyes-Face, Arms, Speech, Time (BE-FAST) and Face, Arms, Speech, Time (FAST) in Identifying Posterior Circulation Strokes.J Clin Med. 2024 Oct 3;13(19):5912. doi: 10.3390/jcm13195912. J Clin Med. 2024. PMID: 39407971 Free PMC article.
-
A Glance at Archives of Academic Emergency Medicine Journal in 2024.Arch Acad Emerg Med. 2024 Nov 19;13(1):e0. doi: 10.22037/aaem.v13i1.2571. eCollection 2025. Arch Acad Emerg Med. 2024. PMID: 40487906 Free PMC article. No abstract available.
-
Cincinnati Prehospital Stroke Scale (CPSS) as a Screening Tool for Early Identification of Cerebral Large Vessel Occlusions; a Systematic Review and Meta-analysis.Arch Acad Emerg Med. 2024 Mar 26;12(1):e38. doi: 10.22037/aaem.v12i1.2242. eCollection 2024. Arch Acad Emerg Med. 2024. PMID: 38737135 Free PMC article. Review.
References
-
- Nogueira RG, Jadhav AP, Haussen DC, Bonafe A, Budzik RF, Bhuva P, et al. Thrombectomy 6 to 24 Hours after Stroke with a Mismatch between Deficit and Infarct. N Engl J Med. 2018;378(1):11–21. - PubMed
-
- Powers WJ, Derdeyn CP, Biller J, Coffey CS, Hoh BL, Jauch EC, et al. 2015 American Heart Association/American Stroke Association Focused Update of the 2013 Guidelines for the Early Management of Patients With Acute Ischemic Stroke Regarding Endovascular Treatment: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke. 2015;46(10):3020–35. - PubMed
Publication types
LinkOut - more resources
Full Text Sources