

Rapid progression from complete molar pregnancy to post-molar gestational trophoblastic neoplasia: a rare case report and literature review
- PMID: 38162509
- PMCID: PMC10757842
- DOI: 10.3389/fonc.2023.1303249
Rapid progression from complete molar pregnancy to post-molar gestational trophoblastic neoplasia: a rare case report and literature review
Abstract
Background: Post-molar gestational trophoblastic neoplasia (pGTN) develops in about 15% to 20% of complete hydatidiform mole (CMH). Commonly, pGTN is diagnosed based on hCG monitoring following the molar evacuation. To date, no detailed information is available on how fast can pGTN develop from CHM. However, the concurrence of CHM and pGTN is extremely rare.
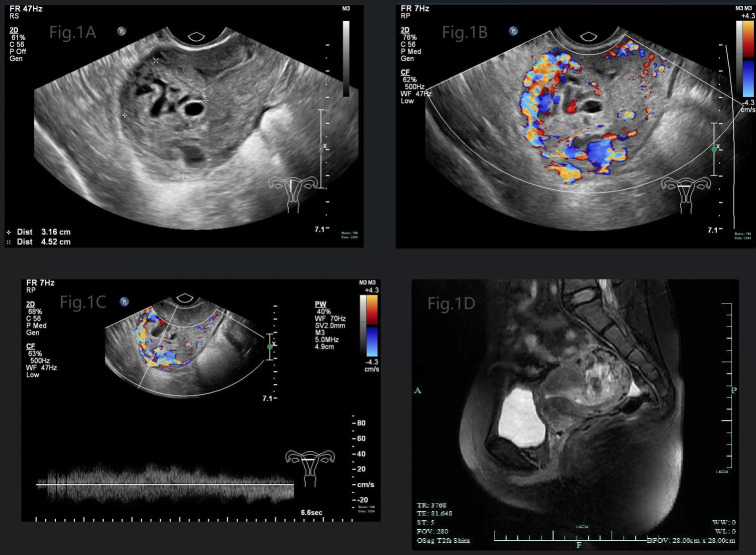
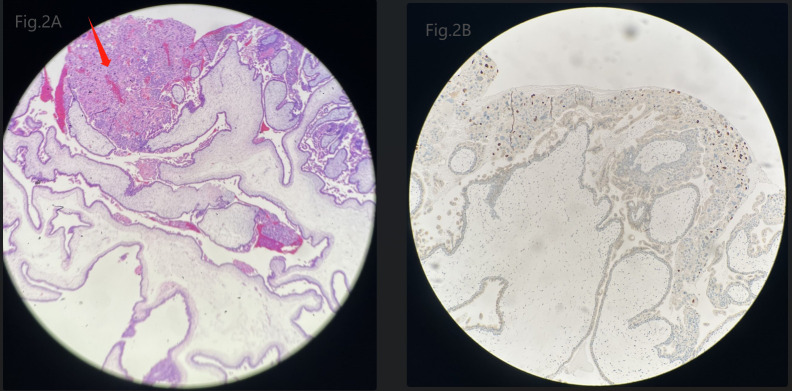
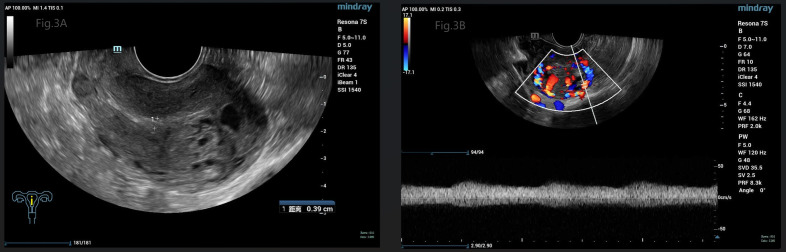
Case presentation: A 29-year-old woman presented to the gynecology department with irregular vaginal bleeding and an elevated hCG serum level. Both ultrasound and MRI showed heterogeneous mass in uterine cavity and myometrium. Suction evacuation was performed and histologic examination of the evacuated specimen confirmed complete hydatidiform mole. Repeated ultrasound showed significant enlargement of the myometrium mass one week after the evacuation. pGTN with prognostic score of 4 was then diagnosed and multi-agent chemotherapy regimen implemented with a good prognosis.
Conclusion: In rare cases, CMH can rapidly progress into pGTN. Imaging in combination with hCG surveillance seems to play a vital role guiding timely diagnosis and treatment in the specific condition. Low-risk gestational trophoblastic neoplasia (GTN) should be managed stratified according to the individual situation.
Keywords: complete hydatidiform mole; gestational trophoblastic disease; gestational trophoblastic tumor; hydatidiform mole; ultrasound.
Copyright © 2023 Qian, Gracious and Sun.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
What is the optimal duration of human chorionic gonadotrophin surveillance following evacuation of a molar pregnancy? A retrospective analysis on over 20,000 consecutive patients.Gynecol Oncol. 2018 Feb;148(2):254-257. doi: 10.1016/j.ygyno.2017.12.008. Epub 2017 Dec 9. Gynecol Oncol. 2018. PMID: 29229282
-
A Case of Rapid Transformation from Hydatidiform Mole to Invasive Mole: The Importance of β-hCG (Human Chorionic Gonadotropin) Serum Levels in Follow-Up Evaluation.Am J Case Rep. 2021 Jun 15;22:e931156. doi: 10.12659/AJCR.931156. Am J Case Rep. 2021. PMID: 34127641 Free PMC article.
-
The role of single-dose prophylactic methotrexate in the prevention of post-molar gestational trophoblastic neoplasia in patients with high-risk molar pregnancy.BMC Cancer. 2024 Nov 13;24(1):1400. doi: 10.1186/s12885-024-13162-0. BMC Cancer. 2024. PMID: 39538177 Free PMC article.
-
Does a human chorionic gonadotropin level of over 20,000 IU/L four weeks after uterine evacuation for complete hydatidiform mole constitute an indication for chemotherapy for gestational trophoblastic neoplasia?Eur J Obstet Gynecol Reprod Biol. 2018 Apr;223:50-55. doi: 10.1016/j.ejogrb.2018.02.001. Epub 2018 Feb 15. Eur J Obstet Gynecol Reprod Biol. 2018. PMID: 29477553 Review.
-
Diagnosis and outcome of hydatidiform moles in missed-miscarriage: a cohort-study, systematic review and meta-analysis.Eur J Obstet Gynecol Reprod Biol. 2020 Oct;253:206-212. doi: 10.1016/j.ejogrb.2020.07.030. Epub 2020 Aug 1. Eur J Obstet Gynecol Reprod Biol. 2020. PMID: 32877774
Cited by
-
Rapid Progression of Molar Pregnancy to Choriocarcinoma With Pulmonary Metastases.Cureus. 2025 May 4;17(5):e83452. doi: 10.7759/cureus.83452. eCollection 2025 May. Cureus. 2025. PMID: 40462788 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources