

Durable immunity to EBV after rituximab and third-party LMP-specific T cells: a Children's Oncology Group study
- PMID: 38163318
- PMCID: PMC10909726
- DOI: 10.1182/bloodadvances.2023010832
Durable immunity to EBV after rituximab and third-party LMP-specific T cells: a Children's Oncology Group study
Abstract
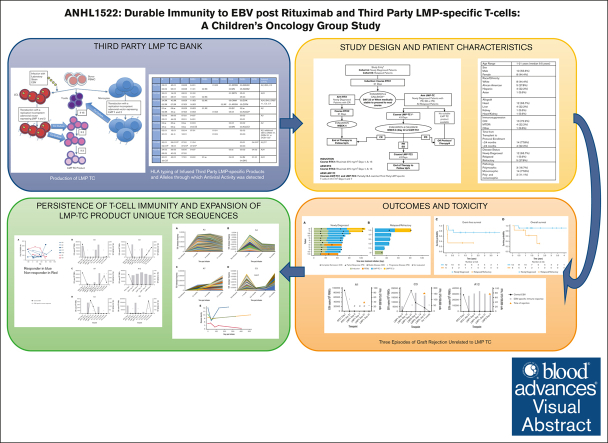
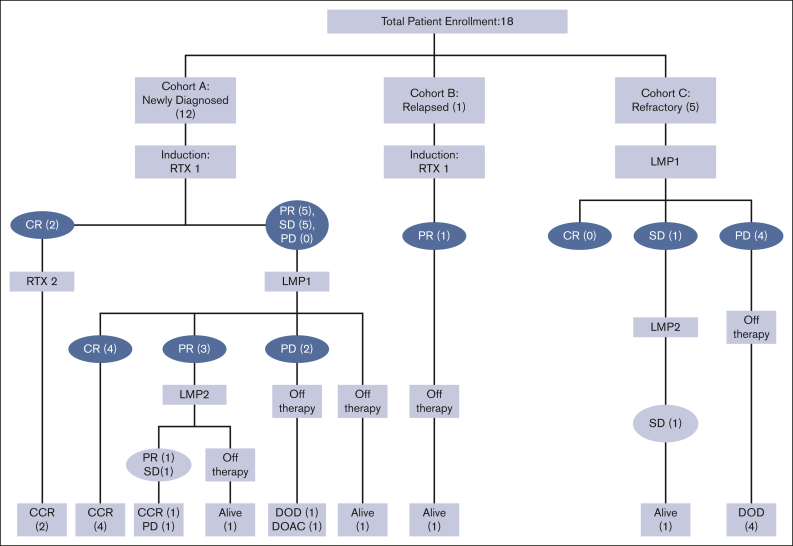
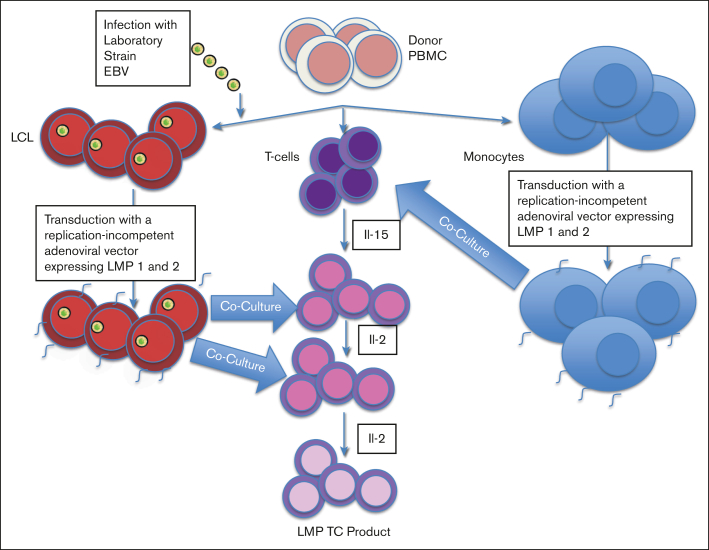
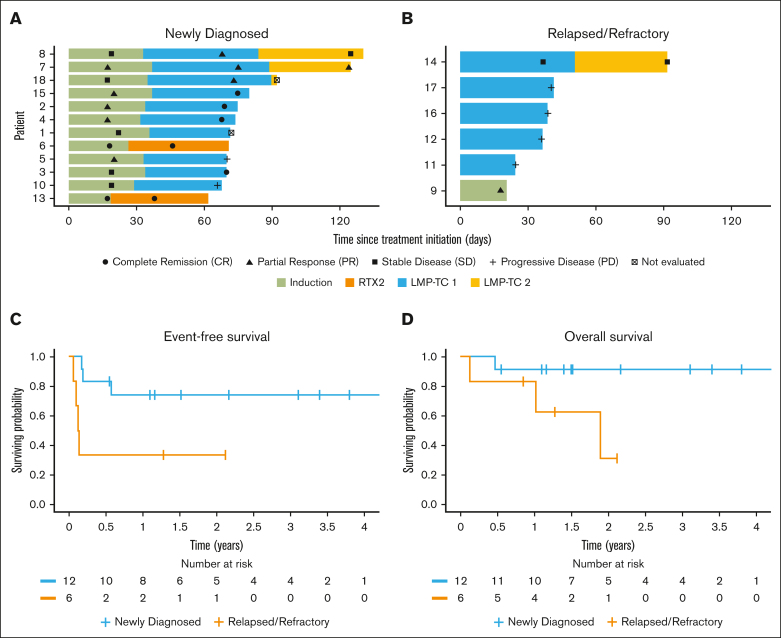
Posttransplant lymphoproliferative disease (PTLD) in pediatric solid organ transplant (SOT) recipients is characterized by uncontrolled proliferation of Epstein-Barr virus-infected (EBV+) B cells due to decreased immune function. This study evaluated the feasibility, safety, clinical and immunobiological outcomes in pediatric SOT recipients with PTLD treated with rituximab and third-party latent membrane protein-specific T cells (LMP-TCs). Newly diagnosed (ND) patients without complete response to rituximab and all patients with relapsed/refractory (R/R) disease received LMP-TCs. Suitable LMP-TC products were available for all eligible subjects. Thirteen of 15 patients who received LMP-TCs were treated within the prescribed 14-day time frame. LMP-TC therapy was generally well tolerated. Notable adverse events included 3 episodes of rejection in cardiac transplant recipients during LMP-TC therapy attributed to subtherapeutic immunosuppression and 1 episode of grade 3 cytokine release syndrome. Clinical outcomes were associated with disease severity. Overall response rate (ORR) after LMP-TC cycle 1 was 70% (7/10) for the ND cohort and 20% (1/5) for the R/R cohort. For all cohorts combined, the best ORR for LMP-TC cycles 1 and 2 was 53% and the 2-year overall survival was 70.7%. vβT-cell receptor sequencing showed persistence of adoptively transferred third-party LMP-TCs for up to 8 months in the ND cohort. This study establishes the feasibility of administering novel T-cell therapies in a cooperative group clinical trial and demonstrates the potential for positive outcomes without chemotherapy for ND patients with PTLD. This trial was registered at www.clinicaltrials.gov as #NCT02900976 and at the Children's Oncology Group as ANHL1522.
© 2024 by The American Society of Hematology. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: C.M.B. is a cofounder and scientific advisory board member of Mana Therapeutics and Catamaran Bio; board member of Cabaletta Bio; has stock in NexImmune and Repertoire Immune Medicines; serves as a data safety monitoring board member for SOBI; and has served on advisory boards for Pfizer, Bristol Myers Squibb, and Roche. C.E.A. serves on advisory boards for SOBI and OPNA, not relevant to this study; and receives study support from Genentech/Roche who manufacture rituximab. P.H. is a cofounder and on the board of directors of Mana Therapeutics; and serves on the adviser boards of Cellevolve, Cellenkos, Discovery Life Sciences, Capsida, and MicrofluidX. The remaining authors declare no competing financial interests.
Figures
Similar articles
-
EBV and post-transplant lymphoproliferative disorder: a complex relationship.Hematology Am Soc Hematol Educ Program. 2024 Dec 6;2024(1):728-735. doi: 10.1182/hematology.2024000583. Hematology Am Soc Hematol Educ Program. 2024. PMID: 39644052 Free PMC article. Review.
-
Chimeric antigen receptor (CAR) T-cell therapy for people with relapsed or refractory diffuse large B-cell lymphoma.Cochrane Database Syst Rev. 2021 Sep 13;9(9):CD013365. doi: 10.1002/14651858.CD013365.pub2. Cochrane Database Syst Rev. 2021. PMID: 34515338 Free PMC article.
-
Epstein-Barr virus-associated post-transplant lymphoproliferative disorders in pediatric transplantation: A prospective multicenter study in the United States.Pediatr Transplant. 2024 Jun;28(4):e14763. doi: 10.1111/petr.14763. Pediatr Transplant. 2024. PMID: 38682750 Free PMC article.
-
Risk and prognosis of posttransplant lymphoproliferative disease in Epstein-Barr virus-seronegative kidney transplant recipients - an observational cohort study from Norway and western Denmark.Am J Transplant. 2025 Jul;25(7):1547-1560. doi: 10.1016/j.ajt.2025.01.035. Epub 2025 Jan 28. Am J Transplant. 2025. PMID: 39884653
-
EBV-specific cytotoxic T lymphocytes for refractory EBV-associated post-transplant lymphoproliferative disorder in solid organ transplant recipients: a systematic review.Transpl Int. 2021 Dec;34(12):2483-2493. doi: 10.1111/tri.14107. Epub 2021 Oct 28. Transpl Int. 2021. PMID: 34510581
Cited by
-
Harnessing Cellular Immunotherapy for EBV-Associated Malignancies: Current Advances and Future Directions.J Cell Mol Med. 2025 May;29(10):e70603. doi: 10.1111/jcmm.70603. J Cell Mol Med. 2025. PMID: 40401927 Free PMC article. Review.
-
EBV and post-transplant lymphoproliferative disorder: a complex relationship.Hematology Am Soc Hematol Educ Program. 2024 Dec 6;2024(1):728-735. doi: 10.1182/hematology.2024000583. Hematology Am Soc Hematol Educ Program. 2024. PMID: 39644052 Free PMC article. Review.
-
Virus-Specific T-Cell Therapy for the Management of Viral Infections in the Immunocompromised.Transfus Med Hemother. 2024 Sep 25;52(1):5-26. doi: 10.1159/000540961. eCollection 2025 Feb. Transfus Med Hemother. 2024. PMID: 39944414 Free PMC article. Review.
-
Celebrating a year of immunotherapy/cell and gene therapy in Blood Advances.Blood Adv. 2024 Dec 24;8(24):6334-6336. doi: 10.1182/bloodadvances.2024015305. Blood Adv. 2024. PMID: 39718780 Free PMC article. No abstract available.
References
-
- Wistinghausen B, Gross TG, Bollard C. Post-transplant lymphoproliferative disease in pediatric solid organ transplant recipients. Pediatr Hematol Oncol. 2013;30(6):520–531. - PubMed
-
- Gross TG, Savoldo B, Punnett A. Posttransplant lymphoproliferative diseases. Pediatr Clin North Am. 2010;57(2):481–503. - PubMed
-
- Cohen JI. Epstein-Barr virus infection. N Engl J Med. 2000;343(7):481–492. - PubMed
-
- Cohen JI. Benign and malignant Epstein-Barr virus-associated B-cell lymphoproliferative diseases. Semin Hematol. 2003;40(2):116–123. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
