

Development and Validation of a Protein Risk Score for Mortality in Heart Failure : A Community Cohort Study
- PMID: 38163367
- PMCID: PMC10958437
- DOI: 10.7326/M23-2328
Development and Validation of a Protein Risk Score for Mortality in Heart Failure : A Community Cohort Study
Abstract
Background: Heart failure (HF) is a complex clinical syndrome with high mortality. Current risk stratification approaches lack precision. High-throughput proteomics could improve risk prediction. Its use in clinical practice to guide the management of patients with HF depends on validation and evidence of clinical benefit.
Objective: To develop and validate a protein risk score for mortality in patients with HF.
Design: Community-based cohort.
Setting: Southeast Minnesota.
Participants: Patients with HF enrolled between 2003 and 2012 and followed through 2021.
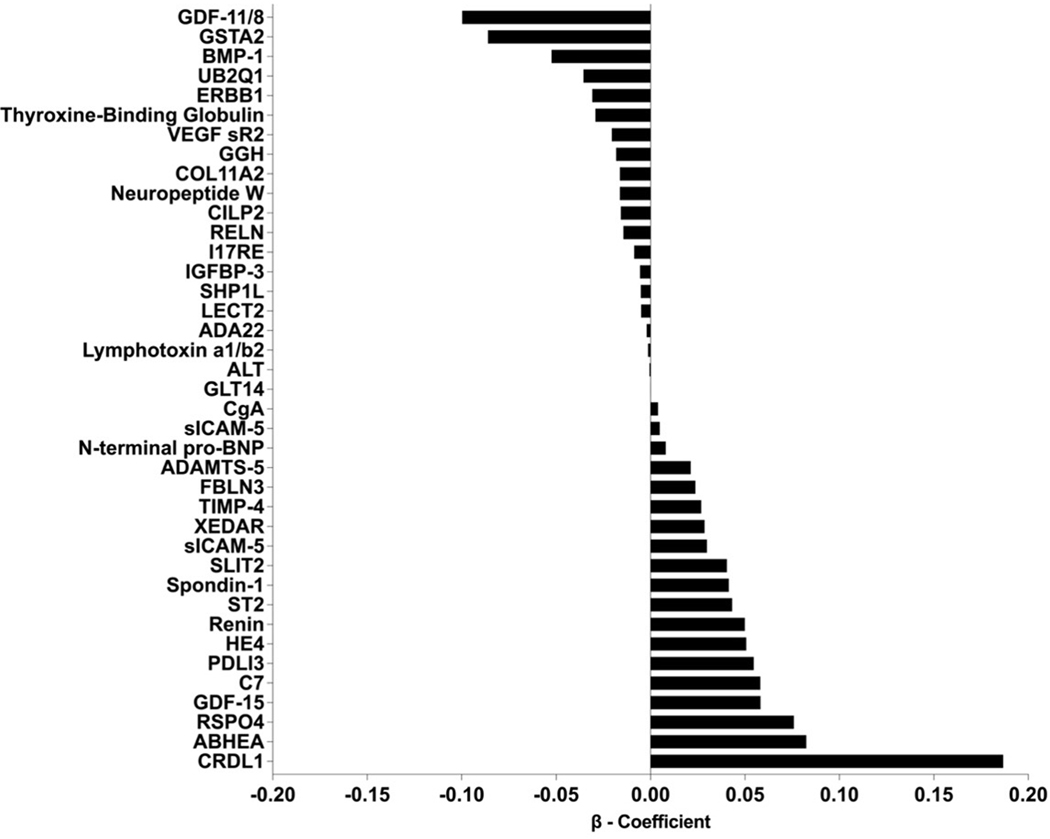
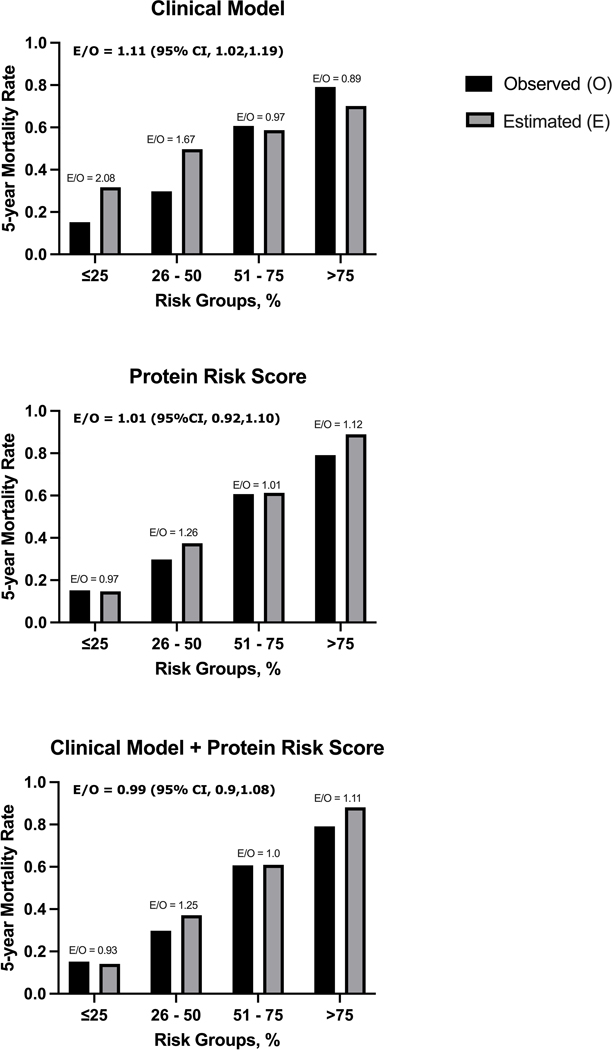
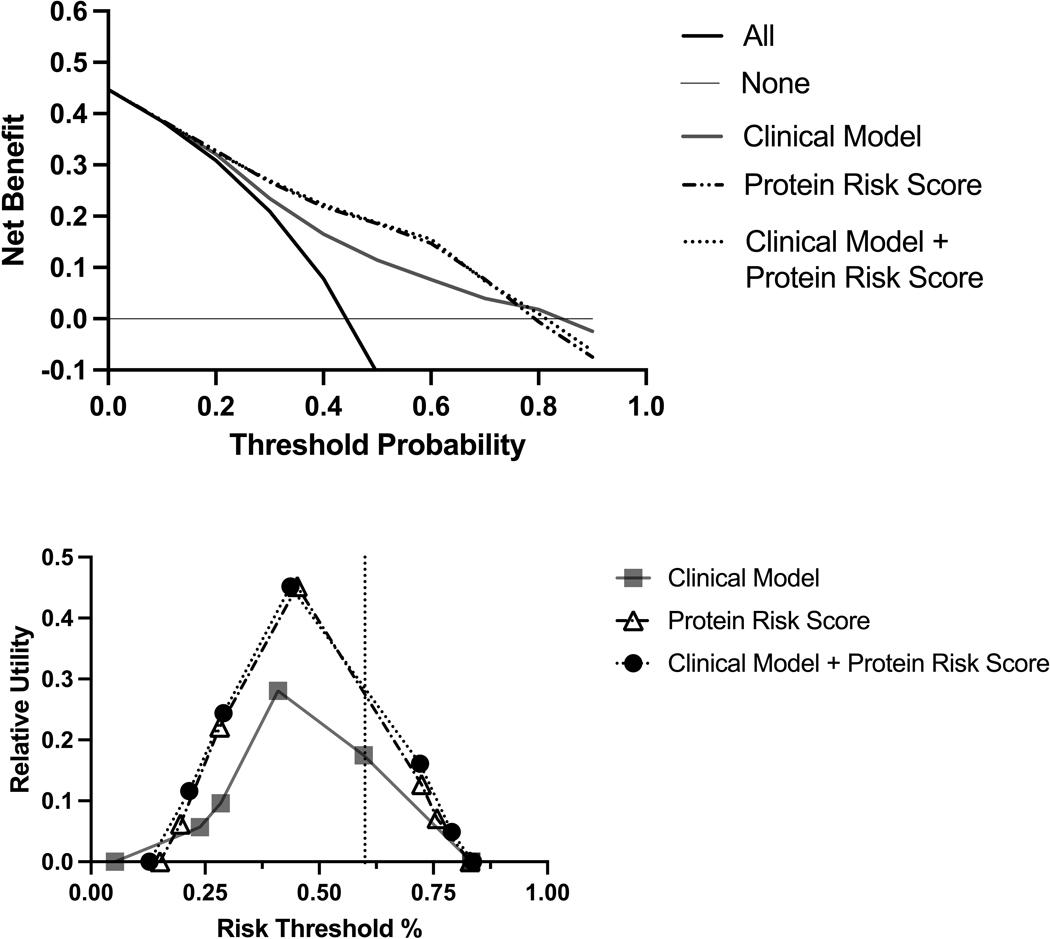
Measurements: A total of 7289 plasma proteins in 1351 patients with HF were measured using the SomaScan Assay (SomaLogic). A protein risk score was derived using least absolute shrinkage and selection operator regression and temporal validation in patients enrolled between 2003 and 2007 (development cohort) and 2008 and 2012 (validation cohort). Multivariable Cox regression was used to examine the association between the protein risk score and mortality. The performance of the protein risk score to predict 5-year mortality risk was assessed using calibration plots, decision curves, and relative utility analyses and compared with a clinical model, including the Meta-Analysis Global Group in Chronic Heart Failure mortality risk score and N-terminal pro-B-type natriuretic peptide.
Results: The development (n = 855; median age, 78 years; 50% women; 29% with ejection fraction <40%) and validation cohorts (n = 496; median age, 76 years; 45% women; 33% with ejection fraction <40%) were mostly similar. In the development cohort, 38 unique proteins were selected for the protein risk score. Independent of ejection fraction, the protein risk score demonstrated good calibration, reclassified mortality risk particularly at the extremes of the risk distribution, and showed greater clinical utility compared with the clinical model.
Limitation: Participants were predominantly of European ancestry, potentially limiting the generalizability of the findings to different patient populations.
Conclusion: Validation of the protein risk score demonstrated good calibration and evidence of predicted benefits to stratify the risk for death in HF superior to that of clinical methods. Further studies are needed to prospectively evaluate the score's performance in diverse populations and determine risk thresholds for interventions.
Primary funding source: Division of Intramural Research at the National Heart, Lung, and Blood Institute of the National Institutes of Health.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous