The Role of Digital Rectal Examination Prostate Volume Category in the Early Detection of Prostate Cancer: Its Correlation with the Magnetic Resonance Imaging Prostate Volume
- PMID: 38164025
- PMCID: PMC10949025
- DOI: 10.5534/wjmh.230028
The Role of Digital Rectal Examination Prostate Volume Category in the Early Detection of Prostate Cancer: Its Correlation with the Magnetic Resonance Imaging Prostate Volume
Abstract
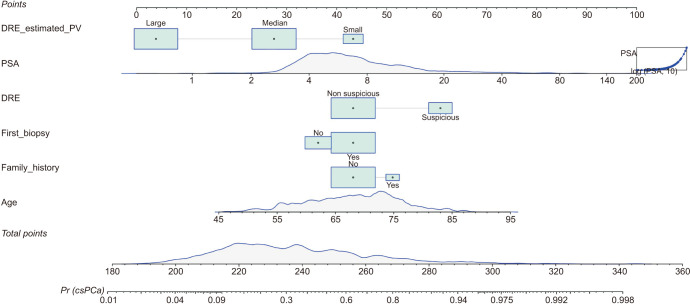
Purpose: To relate the prostate volume category (PVC) assessed with digital rectal examination (DRE)-small, median, and large-and the prostate volumes (PVs) assessed with magnetic resonance imaging (MRI) and transrectal ultrasound (TRUS). To compare the clinically significant prostate cancer (csPCa) discrimination ability of two predictive models based on DRE-PVC and MRI-PV.
Materials and methods: A prospective trial of 2,090 men with prostate-specific antigen >3 ng/mL and/or PCa suspicious DRE were prospectively recruited in 10 centers from Catalonia (Spain), between 2021 and 2022, in whom DRE-PVC was assessed. Pre-biopsy MRI, and 12-core TRUS-random biopsy was always performed after 2- to 6-core TRUS-fusion targeted biopsy of prostate imaging-report and data system >3 lesions. In 370 men (17.7%) the DRE-PVC was unconclusive. Among the 1,720 men finally analyzed the csPCa (grade group >2) detection was 42.4%.
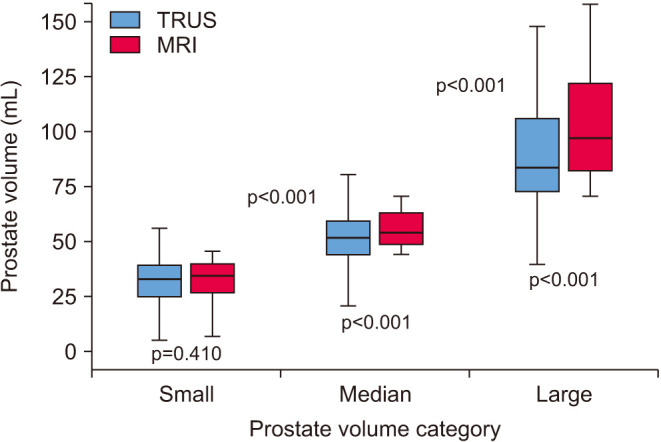
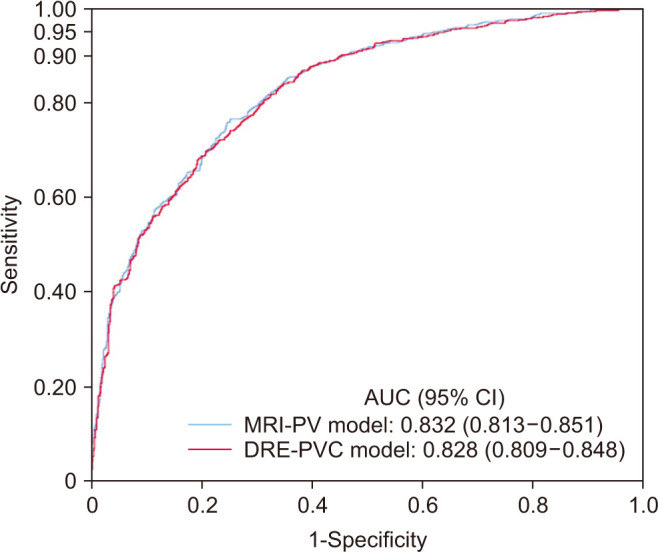
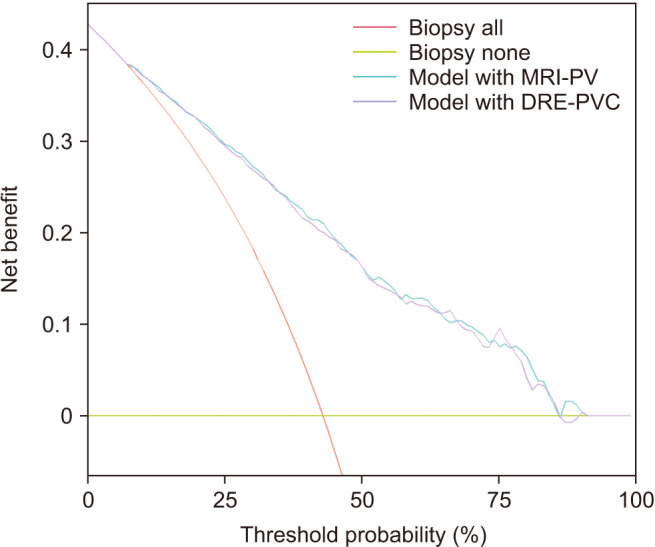
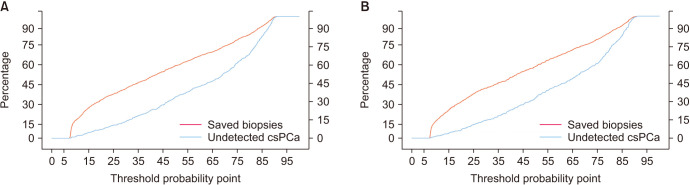
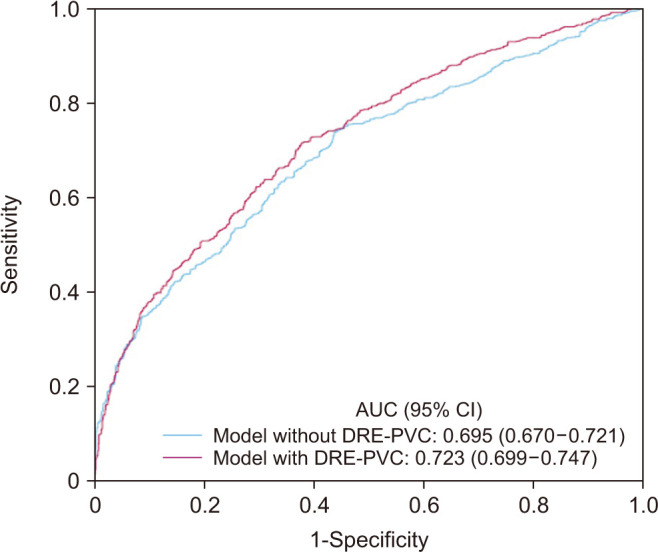
Results: The median (interquartile range) of TRUS and MRI-PVs of small prostates were 33 mL (19-37 mL) and 35 mL (23-30 mL), p=0.410; in median prostates they were 51 mL (38-58 mL) and 55 mL (48-63 mL) respectively, p<0.001; in large prostates 80 mL (60-100 mL) and 95 mL (75-118 mL) respectively, p<0.001. The predictive models sharing the MRI-PV and DRE-PVC showed areas under the curves of 0.832 (95% confidence interval [CI], 0.813-0.851) and 0.828 (95% CI, 0.809-0.848) respectively, p=0.632, as well as similar net benefit and clinical utility.
Conclusions: PVC was unconclusive in 17% of DREs. MRI-PV overestimated the TRUS-PV in median and large prostates. The predictive models based on MRI-PV and DRE-PVC showed similar efficacy to predict csPCa. PVC assessed with DRE is helpful to predict the csPCa risk before MRI.
Keywords: Digital rectal examination; Magnetic resonance imaging; Predictive model; Prostate volume; Prostate volume category; Transrectal ultrasound.
Copyright © 2024 Korean Society for Sexual Medicine and Andrology.
Conflict of interest statement
The authors have nothing to disclose.
Figures
Similar articles
-
A Randomized Controlled Trial To Assess and Compare the Outcomes of Two-core Prostate Biopsy Guided by Fused Magnetic Resonance and Transrectal Ultrasound Images and Traditional 12-core Systematic Biopsy.Eur Urol. 2016 Jan;69(1):149-56. doi: 10.1016/j.eururo.2015.03.041. Epub 2015 Apr 7. Eur Urol. 2016. PMID: 25862143 Clinical Trial.
-
Prostate health index (PHI) and prostate-specific antigen (PSA) predictive models for prostate cancer in the Chinese population and the role of digital rectal examination-estimated prostate volume.Int Urol Nephrol. 2016 Oct;48(10):1631-7. doi: 10.1007/s11255-016-1350-8. Epub 2016 Jun 27. Int Urol Nephrol. 2016. PMID: 27349564
-
Comparison of prostate cancer detection rates between magnetic resonance imaging-targeted biopsy and transrectal ultrasound-guided biopsy according to Prostate Imaging Reporting and Data System in patients with PSA ≥4 ng/mL: a systematic review and meta-analysis.Transl Androl Urol. 2019 Dec;8(6):741-753. doi: 10.21037/tau.2019.12.03. Transl Androl Urol. 2019. PMID: 32038971 Free PMC article.
-
Comparison of Magnetic Resonance Imaging-stratified Clinical Pathways and Systematic Transrectal Ultrasound-guided Biopsy Pathway for the Detection of Clinically Significant Prostate Cancer: A Systematic Review and Meta-analysis of Randomized Controlled Trials.Eur Urol Oncol. 2019 Nov;2(6):605-616. doi: 10.1016/j.euo.2019.05.004. Epub 2019 Jun 14. Eur Urol Oncol. 2019. PMID: 31204311 Free PMC article.
-
Multiparametric MRI in detection and staging of prostate cancer.Dan Med J. 2017 Feb;64(2):B5327. Dan Med J. 2017. PMID: 28157066 Review.
Cited by
-
Validation of the Barcelona-MRI predictive model when PI-RADS v2.1 is used with trans-perineal prostate biopsies.Int Braz J Urol. 2024 Sep-Oct;50(5):595-604. doi: 10.1590/S1677-5538.IBJU.2024.0204. Int Braz J Urol. 2024. PMID: 39106115 Free PMC article.
References
-
- European Commission, Directorate-General for Research and Innovation, Group of Chief Scientific Advisors. Cancer screening in the European Union. Publications Office of the European Union; 2022.
-
- Schoots IG, Padhani AR, Rouvière O, Barentsz JO, Richenberg J. Analysis of magnetic resonance imaging-directed biopsy strategies for changing the paradigm of prostate cancer diagnosis. Eur Urol Oncol. 2020;3:32–41. - PubMed
-
- Sathianathen NJ, Omer A, Harriss E, Davies L, Kasivisvanathan V, Punwani S, et al. Negative predictive value of multiparametric magnetic resonance imaging in the detection of clinically significant prostate cancer in the prostate imaging reporting and data system era: a systematic review and meta-analysis. Eur Urol. 2020;78:402–414. - PubMed
-
- Van Poppel H, Albreht T, Basu P, Hogenhout R, Collen S, Roobol M. Serum PSA-based early detection of prostate cancer in Europe and globally: past, present and future. Nat Rev Urol. 2022;19:562–572. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials