

Long-Term Survival and Cancer Risk in the Hepatitis C Virus-Infected Patients After Antiviral Treatment: A Nationwide Cohort Study
- PMID: 38164272
- PMCID: PMC10751673
- DOI: 10.7150/jca.87259
Long-Term Survival and Cancer Risk in the Hepatitis C Virus-Infected Patients After Antiviral Treatment: A Nationwide Cohort Study
Abstract
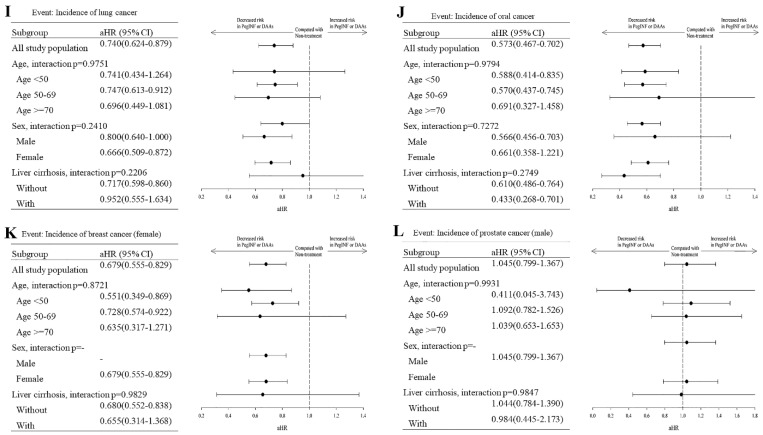
Background: Exposure to the Hepatitis C virus (HCV) has been identified as one of the most critical risk factors for Hepatocellular carcinoma (HCC). Interferons and direct-acting antivirals (DAAs) have been used to treat HCV infection with high rates (95%) of prolonged virological response, a suitable safety profile, and good compliance rates. Methods: We obtained information from Taiwan's Health and Welfare Data Science Center. (HWDSC). In this observational cohort research, patients with HCV who received a diagnosis in Taiwan between 2011 and 2018 were included. Results: 78,300 untreated HCV patients were paired for age, sex, and index date with 39,150 HCV patients who received interferon or DAAs treatment. Compared to the control group, the Interferon or DAAs treatment sample has fewer low-income individuals and more hospitalization requirements. The percentage of kidney illness was reduced in the therapy group compared to the control group, but the treatment group had a greater comorbidity rate of gastric ulcers. Interferon or DAA therapy for HCV-infected patients can substantially lower mortality. All cancer diagnoses after HCV infection with interferon treatment aHR 95% CI = 0.809 (0.774-0.846), Sofosbuvir-based DAA aHR 95% CI = 1.009 (0.737-1.381) and Sofosbuvir free DAA aHR 95% CI = 0.944 (0.584-1.526) showing cancer-protective effects in the INF-treated cohort but not DAA. Conclusion: Following antiviral therapy, women appear to have a more substantial preventive impact than men against pancreatic, colorectal, and lung cancer. Interferon or DAAs treatment effect was more significant in the cirrhotic group.
© The author(s).
Conflict of interest statement
Competing Interests: The authors have declared that no competing interest exists.
Figures



References
LinkOut - more resources
Full Text Sources
