

Pretreatment Non-Invasive Biomarkers as Predictors to Estimate Portal Vein Tumor Thrombosis (PVTT) Risk and Long-Term Survival in HBV-Related Hepatocellular Carcinoma Patients Without PVTT
- PMID: 38164511
- PMCID: PMC10758161
- DOI: 10.2147/JHC.S442487
Pretreatment Non-Invasive Biomarkers as Predictors to Estimate Portal Vein Tumor Thrombosis (PVTT) Risk and Long-Term Survival in HBV-Related Hepatocellular Carcinoma Patients Without PVTT
Abstract
Background: PVTT is a hallmark of advanced hepatocellular carcinoma (HCC). We aim to explore the influence of non-invasive biomarkers on the occurrence of PVTT and develop and validate models for predicting prognosis in HBV-related HCC patients without PVTT.
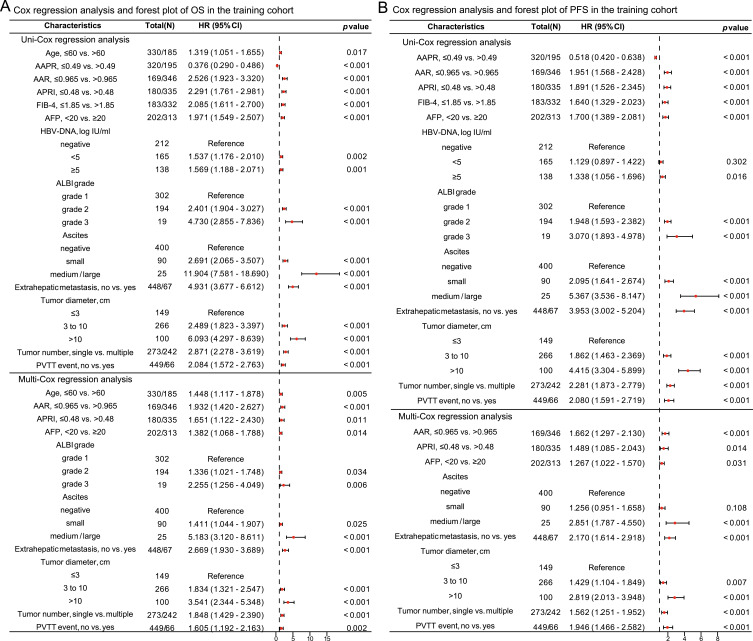
Methods: A total of 1026 HBV-related HCC patients without PVTT were enrolled, with 515 in the training cohort, 216 in the internal validation cohort, and 295 in the external validation cohort. We conducted Cox regression analyses to discern the independent risk factors associated with PVTT events, PFS, and OS, then constructed and validated predictive models. The predictive and discriminatory capabilities of models were assessed using the calibration, time-dependent ROC, and DCA curves.
Results: In our study, 136 patients (13.3%) experienced PVTT events during the follow-up period. The Cox regression analysis unveiled that male gender, AAPR ≤0.49, APRI >0.48, extrahepatic metastasis, and multiple tumors were independent risk factors for PVTT. In the training cohort, non-invasive biomarkers (AAR and APRI), AFP, ascites, and tumor-related characteristics (extrahepatic metastasis, tumor diameter, tumor number, and PVTT event) were independent risk factors for both OS and PFS, whereas age and ALBI grade independently correlated with OS. The C-indexes of OS and PFS nomogram models were 0.795 and 0.733 in the training cohort, 0.765 and 0.716 in the internal validation cohort, and 0.780 and 0.722 in the external validation cohort, respectively. Our models demonstrated strong predictive and discriminative abilities in all cohorts and yielded a greater net benefit compared to three traditional staging systems.
Conclusion: Non-invasive biomarkers are expected to be reliable predictors for assessing PVTT risk and predicting prognosis among HBV-related HCC patients without PVTT.
Keywords: HBV-related HCC; nomogram; non-invasive biomarker; portal vein tumor thrombosis; prognosis.
© 2023 Liu et al.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures





References
LinkOut - more resources
Full Text Sources
