

Predicting anticipated benefit from an extended consultation to personalise care in multimorbidity: a development and internal validation study of a prioritisation algorithm in general practice
- PMID: 38164549
- PMCID: PMC11044021
- DOI: 10.3399/BJGP.2023.0114
Predicting anticipated benefit from an extended consultation to personalise care in multimorbidity: a development and internal validation study of a prioritisation algorithm in general practice
Abstract
Background: Persons with multimorbidity may gain from person-centred care compared with the current protocolised chronic-disease management in Dutch general practice. Given time constraints and limited resources, it is essential to prioritise those most in need of an assessment of person-centred chronic-care needs.
Aim: To develop and validate a prioritisation algorithm based on routine electronic medical record (EMR) data that distinguishes between patients with multimorbidity who would, and those who would not, benefit from an extended person-centred consultation to assess person-centred chronic-care needs, as judged by GPs.
Design and setting: A mixed-methods study was conducted in five general practices in the north-west region of the Netherlands. Four out of the five practices were situated in rural areas.
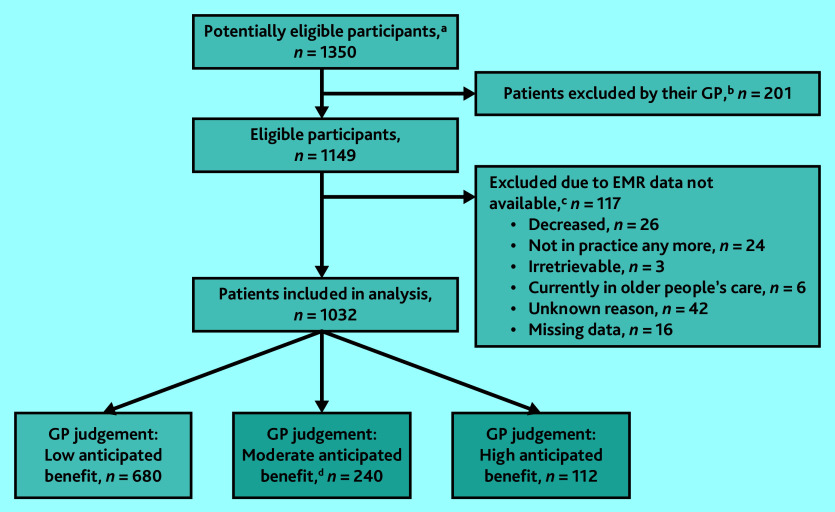
Method: Multivariable logistic regression using EMR data to predict the GPs' judgement on patients' anticipated benefit from an extended consultation, as well as a thematic analysis of a focus group exploring GPs' clinical reasoning for this judgement were conducted. Internal validation was performed using 10-fold cross-validation. Multimorbidity was defined as the presence of ≥3 chronic conditions.
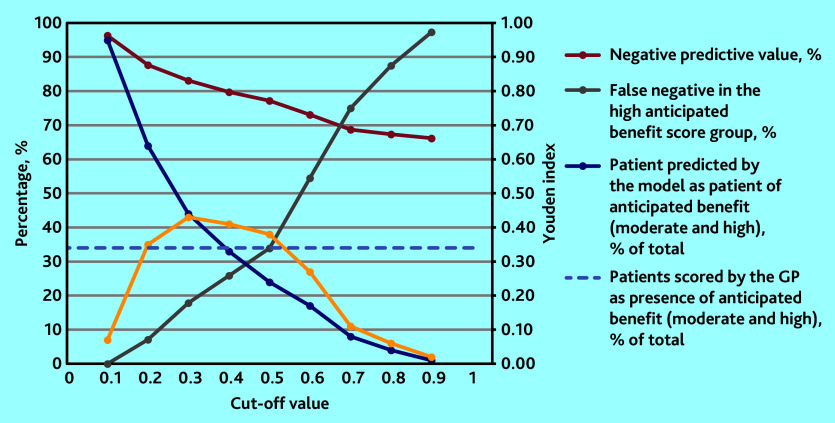
Results: In total, EMRs from 1032 patients were included in the analysis; of these, 352 (34.1%) were judged to have anticipated benefit. The model's cross-validated C-statistic was 0.72 (95% confidence interval = 0.70 to 0.75). Calibration was good. Presence of home visit(s) and history of myocardial infarction were associated with anticipated benefit. Thematic analysis revealed three dimensions feeding anticipated benefit: GPs' cause for concern, patients' mindset regarding their conditions, and balance between received care/expected care needed.
Conclusion: This algorithm may facilitate automated prioritisation, potentially avoiding the need for GPs to personally triage the whole practice population that has multimorbidity. However, external validation of the algorithm and evaluation of actual benefit of consultation is recommended before implementation.
Keywords: general practice; multimorbidity; person-centred care; primary care.
© The Authors.
Conflict of interest statement
The authors have declared no competing interests.
Figures
Similar articles
-
Development of a person-centred care approach for persons with chronic multimorbidity in general practice by means of participatory action research.BMC Prim Care. 2024 Apr 16;25(1):114. doi: 10.1186/s12875-024-02364-x. BMC Prim Care. 2024. PMID: 38627610 Free PMC article.
-
Assessment of functioning in Dutch primary care: Development study of a consultation tool for patients with chronic conditions and multimorbidity.Health Expect. 2022 Aug;25(4):1363-1373. doi: 10.1111/hex.13474. Epub 2022 May 24. Health Expect. 2022. PMID: 35607998 Free PMC article.
-
Identifying high-need patients with multimorbidity from their illness perceptions and personal resources to manage their health and care: a longitudinal study.BMC Fam Pract. 2020 Apr 29;21(1):75. doi: 10.1186/s12875-020-01148-3. BMC Fam Pract. 2020. PMID: 32349683 Free PMC article.
-
General practitioner strategies for managing patients with multimorbidity: a systematic review and thematic synthesis of qualitative research.BMC Fam Pract. 2020 Jul 1;21(1):131. doi: 10.1186/s12875-020-01197-8. BMC Fam Pract. 2020. PMID: 32611391 Free PMC article.
-
Development of a PROM to measure patient-centredness in chronic care consultations in primary care.Health Qual Life Outcomes. 2025 Jan 8;23(1):4. doi: 10.1186/s12955-024-02327-x. Health Qual Life Outcomes. 2025. PMID: 39780227 Free PMC article.
Cited by
-
Concept mapping to promote clinical reasoning in multimorbidity: a mixed methods study in undergraduate family medicine.BMC Med Educ. 2024 Dec 18;24(1):1478. doi: 10.1186/s12909-024-06484-x. BMC Med Educ. 2024. PMID: 39695556 Free PMC article.
References
-
- Fortin M, Bravo G, Hudon C, et al. Relationship between multimorbidity and health-related quality of life of patients in primary care. Qual Life Res. 2006;15(1):83–91. - PubMed
-
- Palmer K, Marengoni A, Forjaz MJ, et al. Multimorbidity care model: recommendations from the consensus meeting of the Joint Action on Chronic Diseases and Promoting Healthy Ageing across the Life Cycle (JA-CHRODIS) Health Policy. 2018;122(1):4–11. - PubMed
-
- Wallace E, Salisbury C, Guthrie B, et al. Managing patients with multimorbidity in primary care. BMJ. 2015;350:h176. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources