

Factors Associated With Successful Extubation Readiness Testing in Children With Congenital Heart Disease
- PMID: 38164566
- PMCID: PMC11108117
- DOI: 10.4187/respcare.11312
Factors Associated With Successful Extubation Readiness Testing in Children With Congenital Heart Disease
Abstract
Background: In children with congenital heart disease, extubation readiness testing (ERT) is performed to evaluate the potential for liberation from mechanical ventilation. There is a paucity of data that suggests what mechanical ventilation parameters are associated with successful ERT. We hypothesized that ERT success would be associated with certain mechanical ventilator parameters.
Methods: Data on daily ERT assessments were recorded as part of a quality improvement project. In accordance with our respiratory therapist-driven ventilator protocol, patients were assessed daily for ERT eligibility and tested daily, if eligible. Mechanical ventilation parameters were categorized a priori to evaluate the differences in levels of respiratory support. The primary outcome was ERT success.
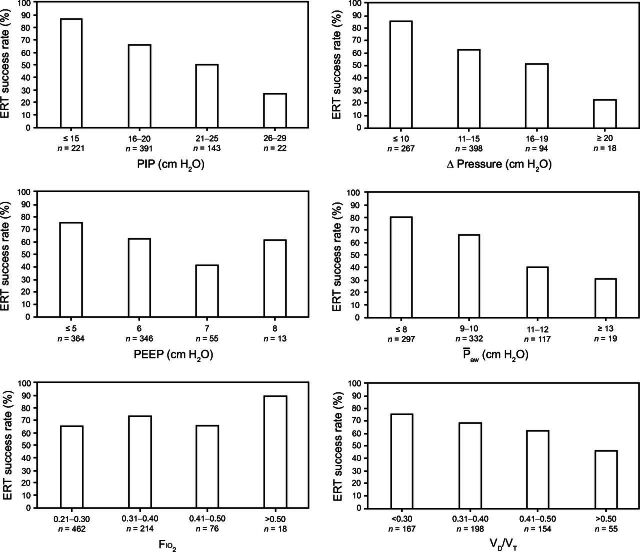
Results: A total of 780 ERTs from 320 subjects (median [interquartile range] age 2.5 [0.6-6.5] months and median weight [interquartile range] 4.2 [3.3-6.9] kg) were evaluated. A total of 528 ERTs (68%) were passed, 306 successful ERTs (58%) resulted in extubation, and 30 subjects (9.4%) were re-intubated. There were statistically significant differences in the ERT pass rate for ventilator mode, peak inspiratory pressure, Δ pressure, PEEP, mean airway pressure ([Formula: see text]), and dead-space-to-tidal-volume ratio (all P < .001) but not for [Formula: see text]. ERT success decreased with increases in peak inspiratory pressure, Δ pressure, PEEP, [Formula: see text], and dead-space-to-tidal-volume ratio. Logistic regression revealed neonates, Δ pressure ≥ 11 cm H2O, and [Formula: see text] > 10 cm H2O were associated with a decreased odds of ERT success, whereas children ages 1-5 years and an [Formula: see text] of 0.31-0.40 had increased odds of ERT success.
Conclusions: ERT pass rates decreased as ventilator support increased; however, some subjects were able to pass ERT despite high ventilator support. We found that [Formula: see text] was associated with ERT success and that protocols should consider using [Formula: see text] instead of PEEP thresholds for ERT eligibility. Cyanotic lesions were not associated with ERT success, which suggests that patients with cyanotic heart disease can be included in ERT protocols.
Keywords: ERT; children; congenital heart disease; extubation; pediatrics; spontaneous breathing trial; ventilator weaning.
Copyright © 2024 by Daedalus Enterprises.
Conflict of interest statement
Mr Miller is a section editor for Respiratory Care and discloses relationships with Saxe Communications, S2N Health, and Fisher & Paykel. Dr Rotta discloses relationships with Vapotherm, Breas US, and Elsevier. The other authors have disclosed no conflicts of interest.
Figures
Similar articles
-
Association Between Pressure Support During Extubation Readiness Testing and Time to First Extubation in Children With Congenital Heart Disease.Respir Care. 2023 Mar;68(3):300-308. doi: 10.4187/respcare.10251. Epub 2022 Nov 22. Respir Care. 2023. PMID: 36414274 Free PMC article.
-
High-Risk Extubation Readiness Testing for Children With Cardiac Critical Illness.Respir Care. 2024 Aug 24;69(9):1108-1115. doi: 10.4187/respcare.11670. Respir Care. 2024. PMID: 38688549 Free PMC article.
-
Ventilator Liberation Practices in Pediatric Cardiac Critical Care.Respir Care. 2025 Mar;70(3):319-326. doi: 10.1089/respcare.12239. Respir Care. 2025. PMID: 40029622
-
Clinical Challenges in Pediatric Ventilation Liberation: A Meta-Narrative Review.Pediatr Crit Care Med. 2022 Dec 1;23(12):999-1008. doi: 10.1097/PCC.0000000000003025. Epub 2022 Jul 14. Pediatr Crit Care Med. 2022. PMID: 35830707 Free PMC article. Review.
-
Executive Summary: International Clinical Practice Guidelines for Pediatric Ventilator Liberation, A Pediatric Acute Lung Injury and Sepsis Investigators (PALISI) Network Document.Am J Respir Crit Care Med. 2023 Jan 1;207(1):17-28. doi: 10.1164/rccm.202204-0795SO. Am J Respir Crit Care Med. 2023. PMID: 36583619 Free PMC article.
Cited by
-
Successful Extubation of Children With Congenital Heart Disease Requires a Specialized Approach.Respir Care. 2024 Mar 27;69(4):521-523. doi: 10.4187/respcare.11949. Respir Care. 2024. PMID: 38538024 Free PMC article. No abstract available.
-
Framework for Research Gaps in Pediatric Ventilator Liberation.Chest. 2024 Nov;166(5):1056-1070. doi: 10.1016/j.chest.2024.05.012. Epub 2024 Jun 7. Chest. 2024. PMID: 38852880
References
-
- Ferreira FV, Sugo EK, Aragon DC, Carmona F, Carlotti APCP. Spontaneous breathing trial for prediction of extubation success in pediatric patients following congenital heart surgery: a randomized, controlled trial. Pediatr Crit Care Med 2019;20(10):940-946. - PubMed
-
- Miura S, Jardim PV, Butt W, Namachivayam SP. Extubation failure and major adverse events secondary to extubation failure following neonatal cardiac surgery. Pediatr Crit Care Med 2020;21(12):e1119-e1125. - PubMed
-
- Venkataraman ST. Liberation from mechanical ventilation after cardiac surgery in infants and children: need for better definitions and approach. Pediatr Crit Care Med 2019;20(10):990-992. - PubMed
-
- Abu-Sultaneh S, Iyer NP, Fernandez A, Gaies M, Gonzalez-Dambrauskas S, Hotz JC, et al. . Executive summary: International Clinical Practice Guidelines for Pediatric Ventilator Liberation, a Pediatric Acute Lung Injury and Sepsis Investigators (PALISI) network document. Am J Respir Crit Care Med 2023;207(1):17-28. - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
