

The Accuracy of Readily Available Consumer-Grade Oxygen Saturation Monitors in Pediatric Patients
- PMID: 38164568
- PMCID: PMC11108112
- DOI: 10.4187/respcare.11258
The Accuracy of Readily Available Consumer-Grade Oxygen Saturation Monitors in Pediatric Patients
Abstract
Background: Pulse oximetry measurement is ubiquitous in acute health care settings in high-income countries and is familiar to any parent whose child has been treated in such a setting. Oximeters for home use are readily available online and are incorporated in several smartphones and smartwatches.
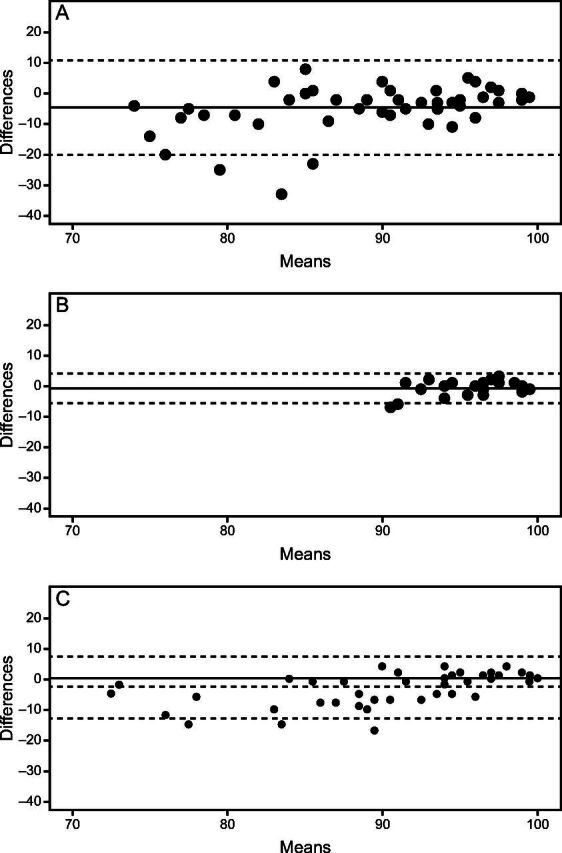
Methods: We wished to determine how accurate are oximeters available online that are designated for adult and pediatric use, and the saturation monitor integrated in a smartphone, when used in children, compared to reference, hospital-grade oximeters. We evaluated a fingertip oximeter marketed for children purchased online; an adult fingertip oximeter purchased online; the oximeter integrated in a smartphone; and reference, hospital-grade oximeters. Participants were < 18 y of age. Bland-Altman charts were generated, and the estimated root mean square error (EARMS) was calculated. Rates of failure to obtain a measurement, relationship between device and time to successful measurement, relationship between age and time to successful measurement, and relationship between error (vs the reference device) and age were evaluated for each consumer-grade device.
Results: We measured SpO2 in 74 children between 0.1-17.0 y of age. Subjects weighing < 30 kg had a median (interquartile range [IQR]) age of 2 (1.0 month-1.4 y) months, and subjects weighing ≥ 30 kg had a median (IQR) age of 14.3 (11.9-16.2) y. Readings could not be obtained in 7.5, 0, and 38.8% of subjects using the pediatric, adult, and smartphone oximeters, respectively. The time to successful reading had a modest negative correlation with age with the inexpensive adult and pediatric oximeters. The inexpensive pediatric oximeter had an overall negative bias, with a mean difference from the reference device of -4.5% (SD 7.9%) and an error that ranged from > 8% to < 33% the reference device. The EARMS was 7.92%. The inexpensive adult oximeter demonstrated no obvious trend in error in the limited saturation range evaluated of 87-99%. The overall mean difference was -0.7% (SD 2.5%). EARMS was 2.5%. The smartphone oximeter underestimated SpO2 at saturations < 94% and overestimated SpO2 for saturations > 94%. Saturations could read as much as > 4%, or < 17%, than the reference oximeter. The mean difference was -2.9% (SD 5.2%). EARMS was 5.1%.
Conclusions: Our findings suggest that the performance of consumer-grade devices varies considerably by both subject age and device. The pediatric fingertip device and smartphone application we tested are poorly suited for use in infants. The adult fingertip device we tested performed quite well in larger children with relatively normal oxygen saturations, and the pediatric fingertip device performed moderately well in subjects > 1 y of age who weighed < 30 kg. Given the vast number of devices available online and ever-changing technology, research to evaluate nonclinical oximeters will continue to be required.
Keywords: child; direct-to-consumer testing; oximetry; pulse; smartphones.
Copyright © 2024 by Daedalus Enterprises.
Conflict of interest statement
The authors have disclosed no conflicts of interest.
Figures
Similar articles
-
Families' perceptions of consumer-grade, inexpensive oxygen saturation monitors.Pediatr Pulmonol. 2024 Dec;59(12):3349-3354. doi: 10.1002/ppul.27203. Epub 2024 Aug 7. Pediatr Pulmonol. 2024. PMID: 39109914 Free PMC article.
-
Evaluation of a New Smartphone Powered Low-cost Pulse Oximeter Device.Ethiop J Health Sci. 2022 Jul;32(4):841-848. doi: 10.4314/ejhs.v32i4.22. Ethiop J Health Sci. 2022. PMID: 35950062 Free PMC article.
-
Accuracy of two pulse oximeters at low arterial hemoglobin-oxygen saturation.Crit Care Med. 1998 Jun;26(6):1128-33. doi: 10.1097/00003246-199806000-00040. Crit Care Med. 1998. PMID: 9635666
-
Potential errors in pulse oximetry. II. Effects of changes in saturation and signal quality.Anaesthesia. 1991 Mar;46(3):207-12. doi: 10.1111/j.1365-2044.1991.tb09411.x. Anaesthesia. 1991. PMID: 2014899 Review.
-
Racial Disparity in Oxygen Saturation Measurements by Pulse Oximetry: Evidence and Implications.Ann Am Thorac Soc. 2022 Dec;19(12):1951-1964. doi: 10.1513/AnnalsATS.202203-270CME. Ann Am Thorac Soc. 2022. PMID: 36166259 Review.
Cited by
-
Advances and Challenges Associated with Low-Cost Pulse Oximeters in Home Care Programs: A Review.Sensors (Basel). 2024 Sep 28;24(19):6284. doi: 10.3390/s24196284. Sensors (Basel). 2024. PMID: 39409324 Free PMC article. Review.
-
When (If) to Worry? Evaluating the Accuracy of Home-Grade Pulse Oximeter Devices.Respir Care. 2024 Mar 27;69(4):516-518. doi: 10.4187/respcare.11960. Respir Care. 2024. PMID: 38538022 Free PMC article. No abstract available.
References
-
- Salyer JW. Neonatal and pediatric pulse oximetry. Respir Care 2003;48(4):386-396. - PubMed
-
- Browne SH, Bernstein M, Bickler PE. Accuracy of Samsung smartphone integrated pulse oximetry meets full FDA clearance standards for clinical use. medRxiv 2021:18.
-
- Modi AM, Kiourkas RD, Li J, Scott JB. Reliability of smartphone pulse oximetry in subjects at risk for hypoxemia. Respir Care 2021;66(3):384-390. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
