

Do patients who read visit notes on the patient portal have a higher rate of "loop closure" on diagnostic tests and referrals in primary care? A retrospective cohort study
- PMID: 38164964
- PMCID: PMC10873783
- DOI: 10.1093/jamia/ocad250
Do patients who read visit notes on the patient portal have a higher rate of "loop closure" on diagnostic tests and referrals in primary care? A retrospective cohort study
Abstract
Objectives: The 2021 US Cures Act may engage patients to help reduce diagnostic errors/delays. We examined the relationship between patient portal registration with/without note reading and test/referral completion in primary care.
Materials and methods: Retrospective cohort study of patients with visits from January 1, 2018 to December 31, 2021, and order for (1) colonoscopy, (2) dermatology referral for concerning lesions, or (3) cardiac stress test at 2 academic primary care clinics. We examined differences in timely completion ("loop closure") of tests/referrals for (1) patients who used the portal and read ≥1 note (Portal + Notes); (2) those with a portal account but who did not read notes (Portal Account Only); and (3) those who did not register for the portal (No Portal). We estimated the predictive probability of loop closure in each group after adjusting for socio-demographic and clinical factors using multivariable logistic regression.
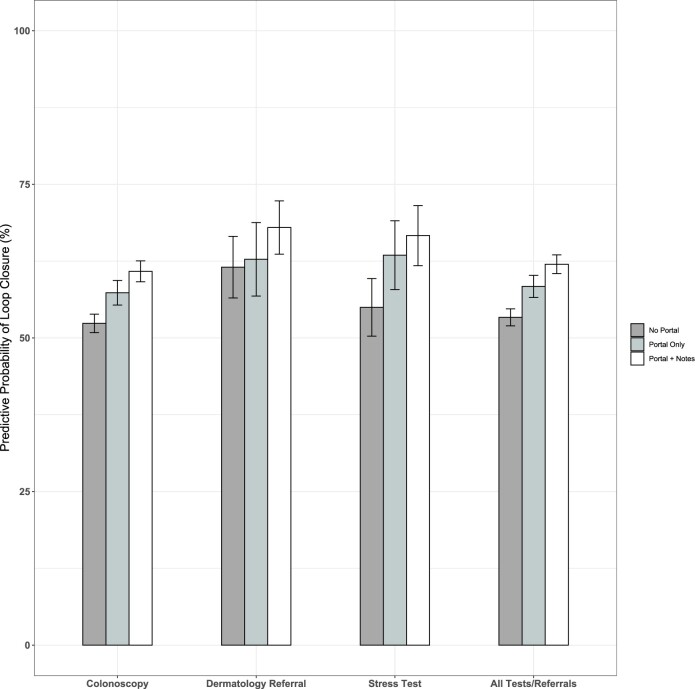
Results: Among 12 849 tests/referrals, loop closure was more common among Portal+Note-readers compared to their counterparts for all tests/referrals (54.2% No Portal, 57.4% Portal Account Only, 61.6% Portal+Notes, P < .001). In adjusted analysis, compared to the No Portal group, the odds of loop closure were significantly higher for Portal Account Only (OR 1.2; 95% CI, 1.1-1.4), and Portal+Notes (OR 1.4; 95% CI, 1.3-1.6) groups. Beyond portal registration, note reading was independently associated with loop closure (P = .002).
Discussion and conclusion: Compared to no portal registration, the odds of loop closure were 20% higher in tests/referrals for patients with a portal account, and 40% higher in tests/referrals for note readers, after controlling for sociodemographic and clinical factors. However, important safety gaps from unclosed loops remain, requiring additional engagement strategies.
Keywords: diagnostic error; diagnostic tests and referrals; patient engagement; patient safety; primary care.
© The Author(s) 2024. Published by Oxford University Press on behalf of the American Medical Informatics Association. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Conflict of interest statement
None declared.
Figures
Similar articles
-
Low Rate of Completion of Recommended Tests and Referrals in an Academic Primary Care Practice with Resident Trainees.Jt Comm J Qual Patient Saf. 2024 Mar;50(3):177-184. doi: 10.1016/j.jcjq.2023.10.005. Epub 2023 Oct 24. Jt Comm J Qual Patient Saf. 2024. PMID: 37996308
-
Frequency and Types of Patient-Reported Errors in Electronic Health Record Ambulatory Care Notes.JAMA Netw Open. 2020 Jun 1;3(6):e205867. doi: 10.1001/jamanetworkopen.2020.5867. JAMA Netw Open. 2020. PMID: 32515797 Free PMC article.
-
The Importance of Visit Notes on Patient Portals for Engaging Less Educated or Nonwhite Patients: Survey Study.J Med Internet Res. 2018 May 24;20(5):e191. doi: 10.2196/jmir.9196. J Med Internet Res. 2018. PMID: 29793900 Free PMC article.
-
Patient and Health Care Provider Perspectives on Patient Access to Test Results via Web Portals: Scoping Review.J Med Internet Res. 2023 Oct 19;25:e43765. doi: 10.2196/43765. J Med Internet Res. 2023. PMID: 37856174 Free PMC article.
-
Patient Portals Facilitating Engagement With Inpatient Electronic Medical Records: A Systematic Review.J Med Internet Res. 2019 Apr 11;21(4):e12779. doi: 10.2196/12779. J Med Internet Res. 2019. PMID: 30973347 Free PMC article.
Cited by
-
Interventions to improve timely cancer diagnosis: an integrative review.Diagnosis (Berl). 2024 Oct 18;12(2):153-162. doi: 10.1515/dx-2024-0113. eCollection 2025 May 1. Diagnosis (Berl). 2024. PMID: 39422050 Free PMC article. Review.
-
Patient and Family Perceptions of Real-Time Access to Electronic Health Information: A Social Media Survey.Appl Clin Inform. 2025 Mar;16(2):327-336. doi: 10.1055/a-2487-7414. Epub 2025 Apr 9. Appl Clin Inform. 2025. PMID: 40204118 Free PMC article.
-
Patient Perspectives on Delayed Specialty Follow-Up After a Primary Care Visit.J Am Board Fam Med. 2025 May 12;38(1):139-153. doi: 10.3122/jabfm.2024.240063R3. J Am Board Fam Med. 2025. PMID: 40268315 Free PMC article.
References
-
- Balogh EP, Miller BT, Ball JR; Committee on Diagnostic Error ICN Health Care; Board on Health Care Services; Institute of Medicine. Improving Diagnosis in Health Care. National Academies Press (US; ); December 29, 2015. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
