

Safety and Efficacy of Nipocalimab in Patients With Generalized Myasthenia Gravis: Results From the Randomized Phase 2 Vivacity-MG Study
- PMID: 38165333
- PMCID: PMC10962909
- DOI: 10.1212/WNL.0000000000207937
Safety and Efficacy of Nipocalimab in Patients With Generalized Myasthenia Gravis: Results From the Randomized Phase 2 Vivacity-MG Study
Abstract
Background and objectives: To evaluate in a phase 2 study the safety and efficacy of IV nipocalimab, a fully human, antineonatal Fc receptor monoclonal antibody, in patients with generalized myasthenia gravis (gMG).
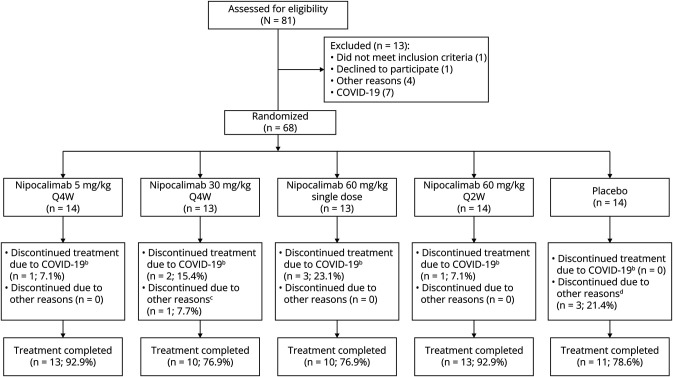
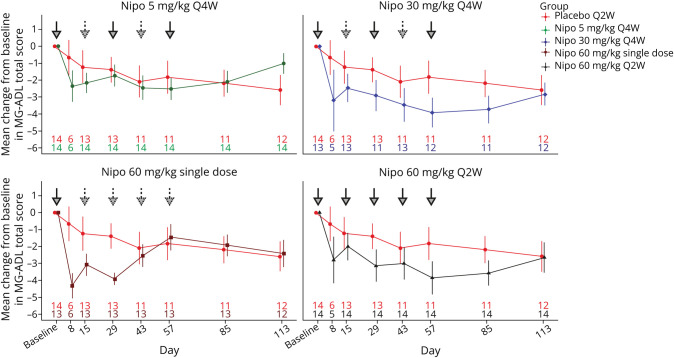
Methods: Patients with gMG with inadequate response to stable standard-of-care (SOC) therapy were randomized 1:1:1:1:1 to receive either IV placebo every 2 weeks (Q2W) or one of 4 IV nipocalimab treatments: 5 mg/kg once every 4 weeks (Q4W), 30 mg/kg Q4W, 60 mg/kg Q2W each for 8 weeks, or a 60 mg/kg single dose, in addition to their background SOC therapy. Infusions (placebo or nipocalimab) were Q2W in all groups to maintain blinding. The primary safety endpoint was incidence of treatment-emergent adverse events (TEAEs), including serious adverse events and adverse events of special interest. The primary efficacy endpoint was change from baseline to day 57 in Myasthenia Gravis-Activities of Daily Living (MG-ADL) total scores. Dose response of change at day 57 was analyzed with a linear trend test over the placebo, nipocalimab 5 mg/kg Q4W, nipocalimab 30 mg/kg Q4W, and nipocalimab 60 mg/kg Q2W groups.
Results: Sixty-eight patients (nipocalimab: n = 54; placebo, n = 14) were randomized; 64 patients (94.1%) were positive for antiacetylcholine receptor autoantibodies, and 4 patients (6%) were positive for antimuscle-specific tyrosine kinase autoantibodies. Fifty-seven patients (83.8%) completed treatment through day 57. The combined nipocalimab group compared with the placebo group demonstrated similar incidences of TEAEs (83.3% vs 78.6%, respectively) and infections (33.3% vs 21.4%, respectively). No deaths or discontinuations due to TEAEs and no TEAEs of special interest (grade ≥3 infection or hypoalbuminemia) were observed with nipocalimab treatment. A statistically significant dose response was observed for change from baseline in MG-ADL at day 57 (p = 0.031, test of linear trend).
Discussion: Nipocalimab was generally safe, well-tolerated, and showed evidence of dose-dependent reduction in MG-ADL scores at day 57 in this phase 2 study. These results support further evaluation of nipocalimab for the treatment of gMG.
Trial registration information: Clinical Trials Registration: NCT03772587; first submitted December 10, 2018; EudraCT Number: 2018-002247-28; first submitted November 30, 2018; date of first patient dosed April 10, 2019.
Classification of evidence: This study provides Class I evidence that for patients with gMG, nipocalimab was well-tolerated, and it did not significantly improve MG-ADL at any individual dose but demonstrated a significant dose response for improved MG-ADL across doses.
Conflict of interest statement
C. Antozzi has received a travel grant from Biogen; J. T. Guptill was a consultant for Momenta Pharmaceuticals and is currently a clinical specialist at Argenx US Inc., USA, full disclosures available at
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous