

Time to Continuous Renal Replacement Therapy Initiation and 90-Day Major Adverse Kidney Events in Children and Young Adults
- PMID: 38165673
- PMCID: PMC10762580
- DOI: 10.1001/jamanetworkopen.2023.49871
Time to Continuous Renal Replacement Therapy Initiation and 90-Day Major Adverse Kidney Events in Children and Young Adults
Abstract
Importance: In clinical trials, the early or accelerated continuous renal replacement therapy (CRRT) initiation strategy among adults with acute kidney injury or volume overload has not demonstrated a survival benefit. Whether the timing of initiation of CRRT is associated with outcomes among children and young adults is unknown.
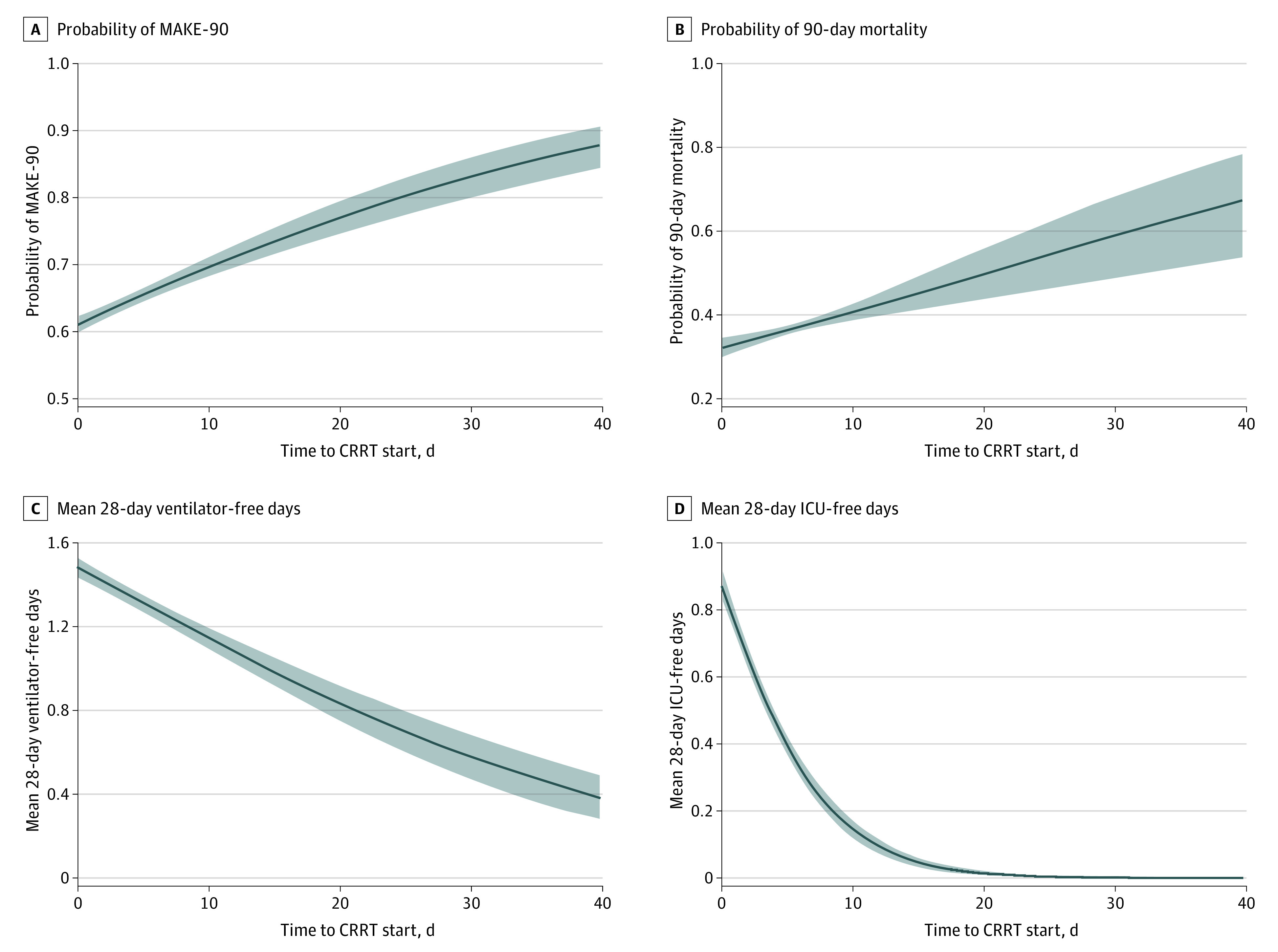
Objective: To determine whether timing of CRRT initiation, with and without consideration of volume overload (VO; <10% vs ≥10%), is associated with major adverse kidney events at 90 days (MAKE-90).
Design, setting, and participants: This multinational retrospective cohort study was conducted using data from the Worldwide Exploration of Renal Replacement Outcome Collaborative in Kidney Disease (WE-ROCK) registry from 2015 to 2021. Participants included children and young adults (birth to 25 years) receiving CRRT for acute kidney injury or VO at 32 centers across 7 countries. Statistical analysis was performed from February to July 2023.
Exposure: The primary exposure was time to CRRT initiation from intensive care unit admission.
Main outcomes and measures: The primary outcome was MAKE-90 (death, dialysis dependence, or persistent kidney dysfunction [>25% decline in estimated glomerular filtration rate from baseline]).
Results: Data from 996 patients were entered into the registry. After exclusions (n = 27), 969 patients (440 [45.4%] female; 16 (1.9%) American Indian or Alaska Native, 40 (4.7%) Asian or Pacific Islander, 127 (14.9%) Black, 652 (76.4%) White, 18 (2.1%) more than 1 race; median [IQR] patient age, 8.8 [1.7-15.0] years) with data for the primary outcome (MAKE-90) were included. Median (IQR) time to CRRT initiation was 2 (1-6) days. MAKE-90 occurred in 630 patients (65.0%), of which 368 (58.4%) died. Among the 601 patients who survived, 262 (43.6%) had persistent kidney dysfunction. Of patients with persistent dysfunction, 91 (34.7%) were dependent on dialysis. Time to CRRT initiation was approximately 1 day longer among those with MAKE-90 (median [IQR], 3 [1-8] days vs 2 [1-4] days; P = .002). In the generalized propensity score-weighted regression, there were approximately 3% higher odds of MAKE-90 for each 1-day delay in CRRT initiation (odds ratio, 1.03 [95% CI, 1.02-1.04]).
Conclusions and relevance: In this cohort study of children and young adults receiving CRRT, longer time to CRRT initiation was associated with greater risk of MAKE-90 outcomes, in particular, mortality. These findings suggest that prospective multicenter studies are needed to further delineate the appropriate time to initiate CRRT and the interaction between CRRT initiation timing and VO to continue to improve survival and reduce morbidity in this population.
Conflict of interest statement
Figures
References
-
- Jetton JG, Boohaker LJ, Sethi SK, et al. ; Neonatal Kidney Collaborative (NKC) . Incidence and outcomes of neonatal acute kidney injury (AWAKEN): a multicentre, multinational, observational cohort study. Lancet Child Adolesc Health. 2017;1(3):184-194. doi: 10.1016/S2352-4642(17)30069-X - DOI - PMC - PubMed
