

Mediation of Age and Thrombectomy Outcome by Neuroimaging Markers of Frailty in Patients With Stroke
- PMID: 38165676
- PMCID: PMC10762575
- DOI: 10.1001/jamanetworkopen.2023.49628
Mediation of Age and Thrombectomy Outcome by Neuroimaging Markers of Frailty in Patients With Stroke
Abstract
Importance: Age is a leading predictor of poor outcomes after brain injuries like stroke. The extent to which age is associated with preexisting burdens of brain changes, visible on neuroimaging but rarely considered in acute decision-making or trials, is unknown.
Objectives: To explore the mediation of age on functional outcome by neuroimaging markers of frailty (hereinafter neuroimaging frailty) in patients with acute ischemic stroke receiving endovascular thrombectomy (EVT).
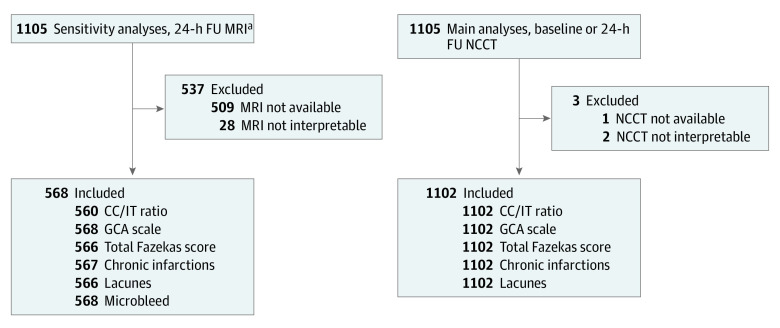
Design, setting, and participants: This cohort study was a post hoc analysis of the Safety and Efficacy of Nerinetide (NA-1) in Subjects Undergoing Endovascular Thrombectomy for Stroke (ESCAPE-NA1) randomized clinical trial, which investigated intravenous (IV) nerinetide in patients who underwent EVT within a 12-hour treatment window. Patients from 48 acute care hospitals in 8 countries (Canada, US, Germany, Korea, Australia, Ireland, UK, and Sweden) were enrolled between March 1, 2017, and August 12, 2019. Markers of brain frailty (brain atrophy [subcortical or cortical], white matter disease [periventricular or deep], and the number of lacunes and chronic infarctions) were retrospectively assessed while reviewers were blinded to other imaging (eg, computed tomography angiography, computed tomography perfusion) or outcome variables. All analyses were done between December 1, 2022, and January 31, 2023.
Exposures: All patients received EVT and were randomized to IV nerinetide (2.6 mg/kg of body weight) and alteplase (if indicated) treatment vs best medical management.
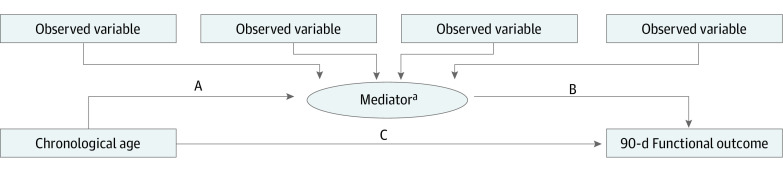
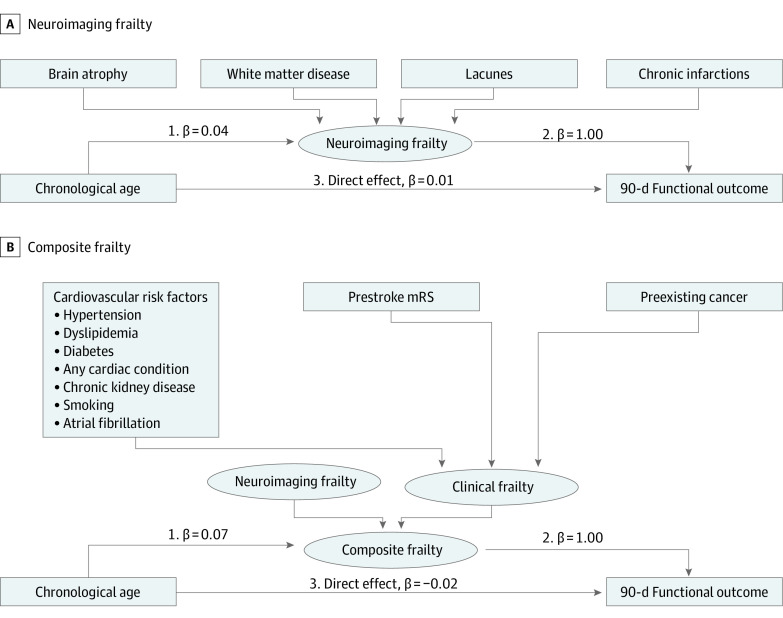
Main outcome and measures: The primary outcome was the proportion of the total effect of age on 90-day outcome, mediated by neuroimaging frailty. A combined mediation was also examined by clinical features associated with frailty and neuroimaging markers (total frailty). Structural equation modeling was used to create latent variables as potential mediators, adjusting for baseline, early ischemic changes; stroke severity; onset-to-puncture time; nerinetide treatment; and alteplase treatment.
Results: Among a total of 1105 patients enrolled in the study, 1102 (median age, 71 years [IQR, 61-80 years]; 554 [50.3%] male) had interpretable imaging at baseline. Of these participants, 549 (49.8%) were treated with IV nerinetide. The indirect effect of age on 90-day outcome, mediated by neuroimaging frailty, was associated with 85.1% of the total effect (β coefficient, 0.04 per year [95% CI, 0.02-0.06 per year]; P < .001). When including both frailty constructs, the indirect pathway was associated with essentially 100% of the total effect (β coefficient, 0.07 per year [95% CI, 0.03-0.10 per year]; P = .001).
Conclusions and relevance: In this cohort study, a secondary analysis of the ESCAPE-NA1 trial, most of the association between age and 90-day outcome was mediated by neuroimaging frailty, underscoring the importance of features like brain atrophy and small vessel disease, as opposed to chronological age alone, in predicting poststroke outcomes. Future trials could include such frailty features to stratify randomization or improve adjustment in outcome analyses.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
