

Efficacy of preoperative lymphoscintigraphy in predicting surgical outcomes of lymphaticovenous anastomosis in lower extremity lymphedema: Clinical correlations in gynecological cancer-related lymphedema
- PMID: 38165945
- PMCID: PMC10760657
- DOI: 10.1371/journal.pone.0296466
Efficacy of preoperative lymphoscintigraphy in predicting surgical outcomes of lymphaticovenous anastomosis in lower extremity lymphedema: Clinical correlations in gynecological cancer-related lymphedema
Abstract
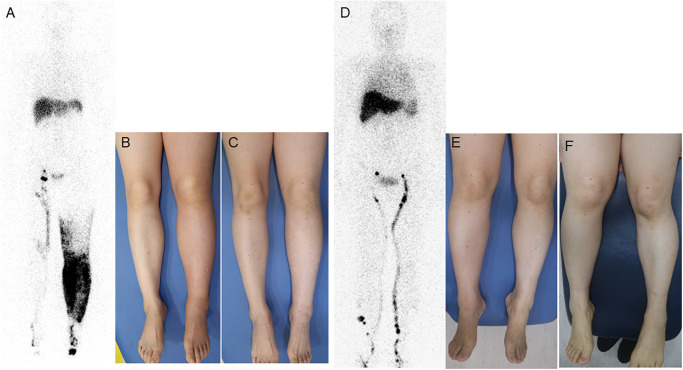
Background: Lymphaticovenous anastomosis (LVA) is a promising microsurgical treatment for lower extremity lymphedema (LEL). Lymphoscintigraphy effectively assesses lower limb lymphatic systems before LVA, but its role in predicting the therapeutic outcomes of LVA is indeterminate. In this study we investigate the efficacy of preoperative lymphoscintigraphy using clinical findings to predict outcomes in gynecological cancer-related LEL patients who underwent LVA.
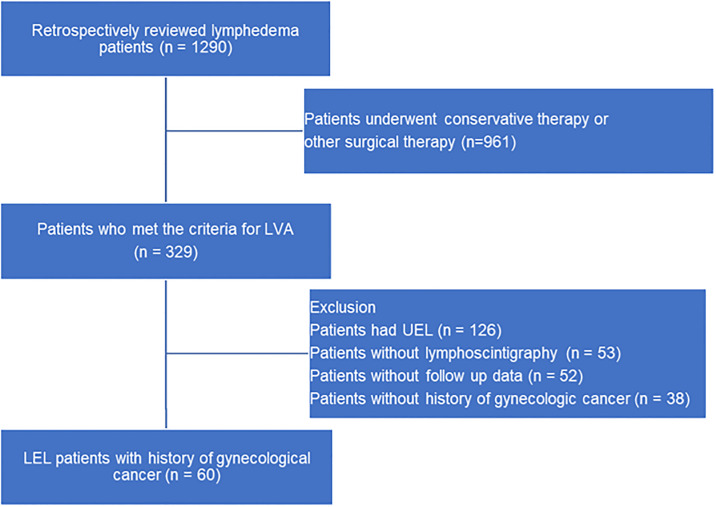
Methods: A retrospective review was conducted on consecutive gynecological cancer patients with LEL who had undergone LVA between June 2018 and June 2021. The therapeutic efficacy was assessed by measuring the change rate of the lower extremity lymphedema index (LELi) six months after surgery. Clinical data and lymphoscintigraphic findings were analyzed to assess therapeutic efficacy of LVA.
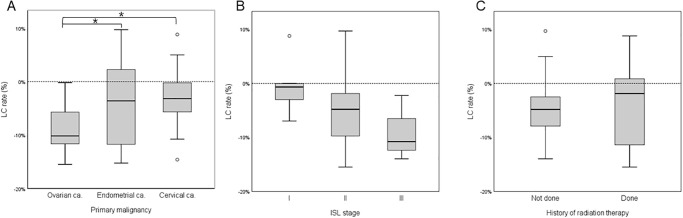
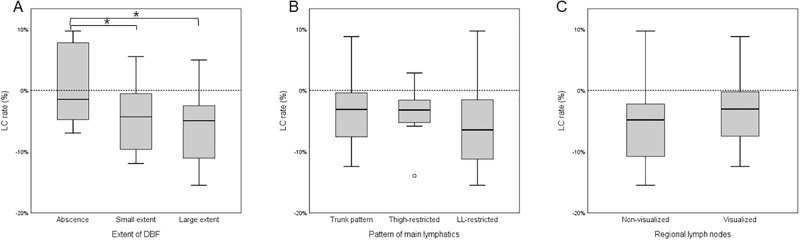
Results: Out of the 60 evaluated legs, 83.3% of the legs showed improved results after LVA. Univariable linear regression analysis revealed that higher preoperative LELi, and ovarian cancer were associated with superior LELi change rate (LC rate). Absence of dermal backflow (DBF) on lymphoscintigraphy was associated with inferior LC rate. Multivariable linear regression analysis identified ovarian cancer and higher preoperative LELi were independently correlated with favorable outcomes, while the absence of DBF was independently correlated with inferior outcomes.
Conclusion: The results of this study emphasizes the effectiveness of preoperative lymphoscintigraphy, preoperative LELi, and primary malignancy as predictors of LVA outcomes in gynecological cancer-related LEL patients.
Copyright: © 2024 Yoo et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Predicting the Outcome of Lymphovenous Anastomosis for Lower Extremity Lymphedema through Lymphoscintigraphy.Int J Med Sci. 2025 Jun 23;22(13):3174-3181. doi: 10.7150/ijms.111506. eCollection 2025. Int J Med Sci. 2025. PMID: 40765558 Free PMC article.
-
Lymphoscintigraphic Findings as Indicators of Lymphaticovenous Anastomosis Outcome in Patients With Extremity Lymphedema: A Retrospective Cohort Study.Clin Nucl Med. 2021 Jul 1;46(7):549-555. doi: 10.1097/RLU.0000000000003630. Clin Nucl Med. 2021. PMID: 33826571
-
Concordance between preoperative imaging methods in patients with limb lymphedema undergoing supermicrosurgical lymphaticovenular anastomosis.J Vasc Surg Venous Lymphat Disord. 2024 Nov;12(6):101891. doi: 10.1016/j.jvsv.2024.101891. Epub 2024 Apr 15. J Vasc Surg Venous Lymphat Disord. 2024. PMID: 38631506 Free PMC article.
-
Lymphaticovenous Anastomosis for Lower Extremity Lymphedema: A Systematic Review.Indian J Plast Surg. 2020 Mar;53(1):17-24. doi: 10.1055/s-0040-1709372. Epub 2020 Apr 17. Indian J Plast Surg. 2020. PMID: 32367914 Free PMC article. Review.
-
A Systematic Stepwise Method to Perform a Supermicrosurgical Lymphovenous Anastomosis.Ann Plast Surg. 2022 May 1;88(5):524-532. doi: 10.1097/SAP.0000000000003023. Epub 2021 Oct 8. Ann Plast Surg. 2022. PMID: 34670962 Review.
Cited by
-
Predicting the Outcome of Lymphovenous Anastomosis for Lower Extremity Lymphedema through Lymphoscintigraphy.Int J Med Sci. 2025 Jun 23;22(13):3174-3181. doi: 10.7150/ijms.111506. eCollection 2025. Int J Med Sci. 2025. PMID: 40765558 Free PMC article.
-
[An overview of integrated surgical management for secondary lower limb lymphedema guided by algorithms].Zhonghua Shao Shang Yu Chuang Mian Xiu Fu Za Zhi. 2025 Jun 20;41(6):516-524. doi: 10.3760/cma.j.cn501225-20250217-00067. Zhonghua Shao Shang Yu Chuang Mian Xiu Fu Za Zhi. 2025. PMID: 40480841 Free PMC article. Chinese.
-
Comparison of the rate of concomitant proximal venous stenosis between the upper and lower extremities in patients with secondary lymphedema undergoing lymphaticovenous anastomosis.J Vasc Surg Venous Lymphat Disord. 2025 Jan;13(1):101947. doi: 10.1016/j.jvsv.2024.101947. Epub 2024 Jul 14. J Vasc Surg Venous Lymphat Disord. 2025. PMID: 39013516 Free PMC article.
References
-
- Beesley VL, Rowlands IJ, Hayes SC, Janda M, O’Rourke P, Marquart L et al. Incidence, risk factors and estimates of a woman’s risk of developing secondary lower limb lymphedema and lymphedema-specific supportive care needs in women treated for endometrial cancer. Gynecol Oncol. 2015;136(1):87–93. doi: 10.1016/j.ygyno.2014.11.006 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
