

Impact of comorbidities in COPD clinical control criteria. The CLAVE study
- PMID: 38166965
- PMCID: PMC10759491
- DOI: 10.1186/s12890-023-02758-0
Impact of comorbidities in COPD clinical control criteria. The CLAVE study
Abstract
Background: Chronic obstructive pulmonary disease (COPD) frequently coexists with other chronic diseases, namely comorbidities. They negatively impact prognosis, exacerbations and quality of life in COPD patients. However, no studies have been performed to explore the impact of these comorbidities on COPD clinical control criteria.
Research question: Determine the relationship between individualized comorbidities and COPD clinical control criteria.
Study design and methods: Observational, multicenter, cross-sectional study performed in Spain involving 4801 patients with severe COPD (< 50 predicted forced expiratory volume in the first second [FEV1%]). Clinical control criteria were defined by the combination of COPD assessment test (CAT) scores (≤16 vs ≥17) and exacerbations in the previous three months (none vs ≥1). Binary logistic regression adjusted by age and FEV1% was performed to identify comorbidities potentially associated with the lack of control of COPD. Secondary endpoints were the relationship between individualized comorbidities with COPD assessment test and exacerbations within the last three months.
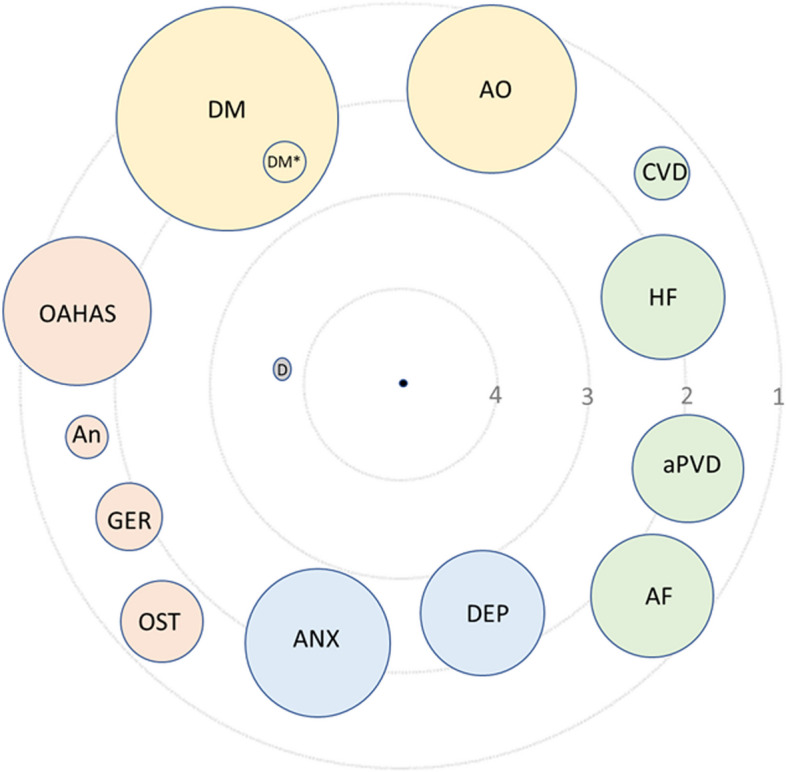
Results: Most frequent comorbidities were arterial hypertension (51.2%), dyslipidemia (36.0%), diabetes (24.9%), obstructive sleep apnea-hypopnea syndrome (14.9%), anxiety (14.1%), heart failure (11.6%), depression (11.8%), atrial fibrillation (11.5%), peripheral arterial vascular disease (10.4%) and ischemic heart disease (10.1%). After age and FEV1% adjustment, comorbidities related to lack of clinical control were cardiovascular diseases (heart failure, peripheral vascular disease and atrial fibrillation; p < 0.0001), psychologic disorders (anxiety and depression; all p < 0.0001), metabolic diseases (diabetes, arterial hypertension and abdominal obesity; all p < 0.001), sleep disorders (p < 0.0001), anemia (p = 0.015) and gastroesophageal reflux (p < 0.0001). These comorbidities were also related to previous exacerbations and COPD assessment test scores.
Interpretation: Comorbidities are frequent in patients with severe COPD, negatively impacting COPD clinical control criteria. They are related to health-related quality of life measured by the COPD assessment test. Our results suggest that comorbidities should be investigated and treated in these patients to improve their clinical control.
Take-home points: Study question: What is the impact of comorbidities on COPD clinical control criteria?
Results: Among 4801 patients with severe COPD (27.5% controlled and 72.5% uncontrolled), after adjustment by age and FEV1%, comorbidities related to lack of clinical control were cardiovascular diseases (heart failure, peripheral vascular disease and atrial fibrillation; p < 0.0001), psychologic disorders (anxiety and depression; p < 0.0001), metabolic diseases (diabetes, arterial hypertension and abdominal obesity; p < 0.001), obstructive sleep apnea-hypopnea syndrome (p < 0.0001), anaemia (p = 0.015) and gastroesophageal reflux (p < 0.0001), which were related to previous exacerbations and COPD assessment test scores.
Interpretation: Comorbidities are related to health-related quality of life measured by the COPD assessment test scores and history of exacerbations in the previous three months.
Keywords: CAT: COPD assessment test; COPD: Chronic obstructive pulmonary disease; Charlson index; Clinical control criteria; Comorbidities; Exacerbations.
© 2023. The Author(s).
Conflict of interest statement
Pere Almagro declares he has received speaking or advisory fees, or economic aid to attend congresses from Astra-Zeneca, GSK, Novartis, Chiesi, Menarini, Boehringer-Ingelheim, Ferrer, and Rovi. Borja G Cosío declares he has received speaking or advisory fees, or economic aid to attend congresses from Astra-Zeneca, GSK, Novartis, Chiesi, Mundipharma, Menarini, Sanofi, TEVA, Boehringer-Ingelheim, and Rovi. He also reports non-financial support from Separ. Juan José Soler-Cataluña has received speaker fees from AstraZeneca, Bial, Boehringer Ingelheim, Chiesi, GSK, Menarini, and consulting fees from Bial, Boehringer Ingelheim, Chiesi and GSK. Diego González-Segura is an employee of Chiesi España SAU, the sponsor of the study. The authors report no other conflicts of interest in this work.
Figures


References
-
- GOLD Reports, editor. Global Initiative for Chronic Obstructive Lung Disease. GOLD; 2021.
-
- GBD 2015 Mortality and Causes of Death Collaborators Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1459–1544. doi: 10.1016/S0140-6736(16)31012-1. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
