

The efficacy and safety of direct oral anticoagulants compared with vitamin K antagonist in patients with hypertrophic cardiomyopathy and atrial fibrillation
- PMID: 38166972
- PMCID: PMC10759476
- DOI: 10.1186/s12959-023-00562-8
The efficacy and safety of direct oral anticoagulants compared with vitamin K antagonist in patients with hypertrophic cardiomyopathy and atrial fibrillation
Abstract
Background: The benefit-risk profile of direct oral anticoagulants (DOAC) therapy in patients with hypertrophic cardiomyopathy (HCM) and atrial fibrillation (AF) has not been well established yet. This study aimed to evaluate the efficacy and safety of DOAC compared with vitamin K antagonists (VKA) in patients with HCM and AF.
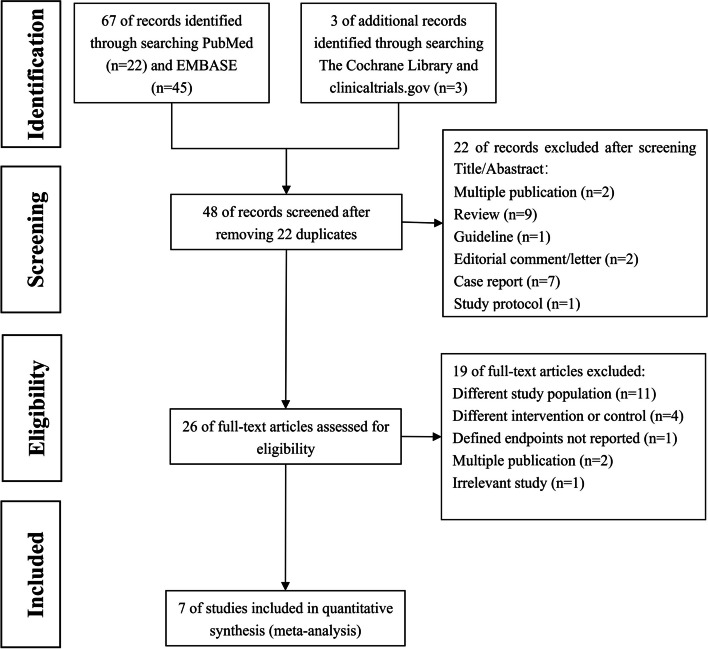
Methods: PubMed, EMBASE, the Cochrane Library, and clinicaltrials.gov were searched to identify studies comparing DOAC with VKA in patients with HCM and AF. The primary endpoint was thromboembolic events. The relative risks and standard errors were pooled by random-effect models using the generic inverse variance method.
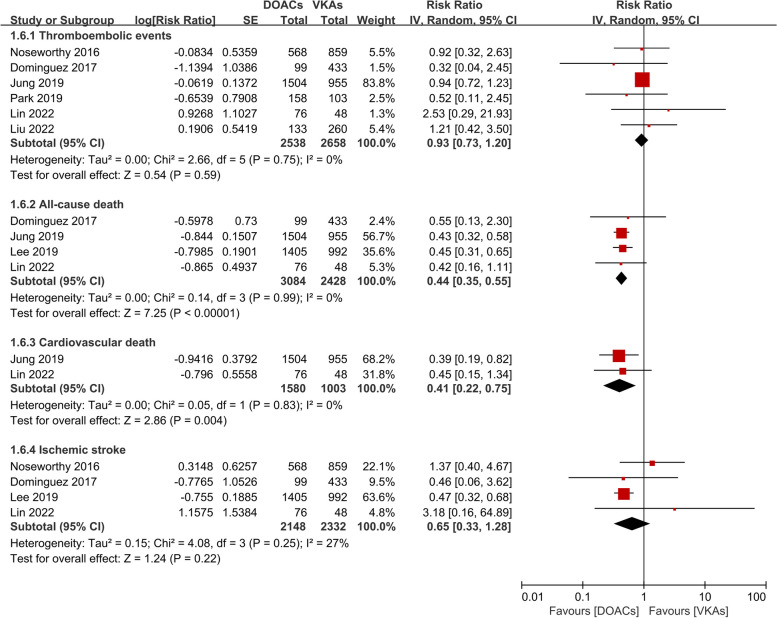
Results: Seven observational studies involving 9395 patients were included in this meta-analysis. Compared to the VKA group, the DOAC group displayed a similar risk of thromboembolic events [RR (95%CI): 0.93 (0.73-1.20), p = 0.59] and ischemic stroke [RR (95%CI): 0.65 (0.33-1.28), p = 0.22]. The incidence of major bleeding was comparable between the two groups [RR (95%CI): 0.75 (0.49-1.15), p = 0.19]. Meanwhile, DOAC therapy was superior to VKA therapy in reducing the incidences of all-cause death [RR (95%CI): 0.44 (0.35-0.55), p < 0.001], cardiovascular death [RR (95%CI): 0.41 (0.22-0.75), p = 0.004], and intracranial hemorrhage [RR (95%CI): 0.42 (0.24-0.74), p = 0.003].
Conclusion: In patients with HCM and AF, DOAC therapy was similar to VKA therapy in reducing the risk of thromboembolic events, without increasing bleeding risk. In addition, the DOAC group displayed significant advantages in reducing mortality and intracranial hemorrhage compared with the VKA group. Further randomized controlled trials are needed to provide more evidence for DOAC therapy in this population.
Keywords: Atrial fibrillation; Direct oral anticoagulants; Hypertrophic cardiomyopathy; Meta-analysis; Vitamin K antagonists.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Maron BJ, Gardin JM, Flack JM, et al. Prevalence of hypertrophic cardiomyopathy in a general population of young adults. Echocardiographic analysis of 4111 subjects in the CARDIA Study. Coronary Artery Risk Development in (Young) Adults. Circulation. 1995;92(4):785–9. 10.1161/01.cir.92.4.785. 10.1161/01.cir.92.4.785 - DOI - PubMed
-
- Elliott PM, Anastasakis A, Borger MA, et al. 2014 ESC guidelines on diagnosis and management of hypertrophic cardiomyopathy: the task force for the diagnosis and Management of Hypertrophic Cardiomyopathy of the European Society of Cardiology (ESC). Eur Heart J. 2014;35(39):2733–79. 10.1093/eurheartj/ehu284. 10.1093/eurheartj/ehu284 - DOI - PubMed
-
- Ommen SR, Mital S, Burke MA, et al. 2020 AHA/ACC guideline for the diagnosis and treatment of patients with hypertrophic cardiomyopathy: a report of the American College of Cardiology/American Heart Association joint committee on clinical practice guidelines. Circulation. 2020;142(25):e558–631. 10.1161/cir.0000000000000937. 10.1161/cir.0000000000000937 - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
