

Impact of radiation doses on clinical relapse of biochemically recurrent prostate cancer after prostatectomy
- PMID: 38167430
- PMCID: PMC10761985
- DOI: 10.1038/s41598-023-50434-4
Impact of radiation doses on clinical relapse of biochemically recurrent prostate cancer after prostatectomy
Abstract
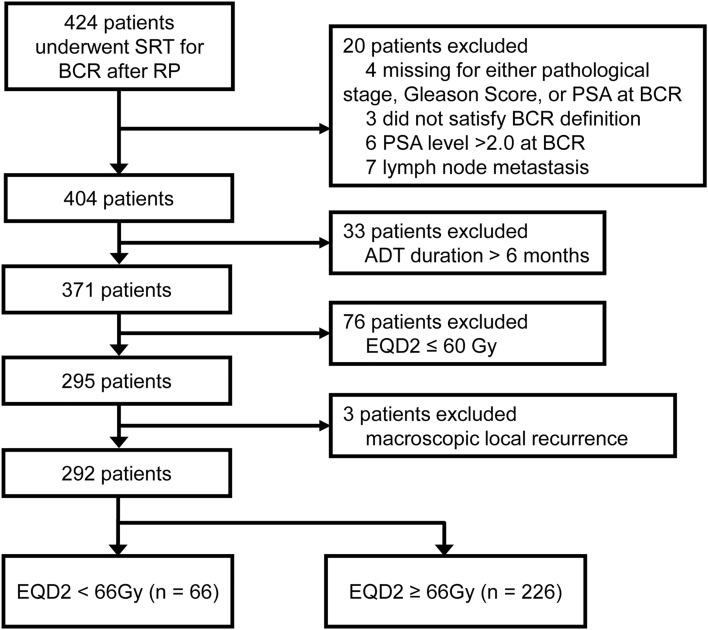
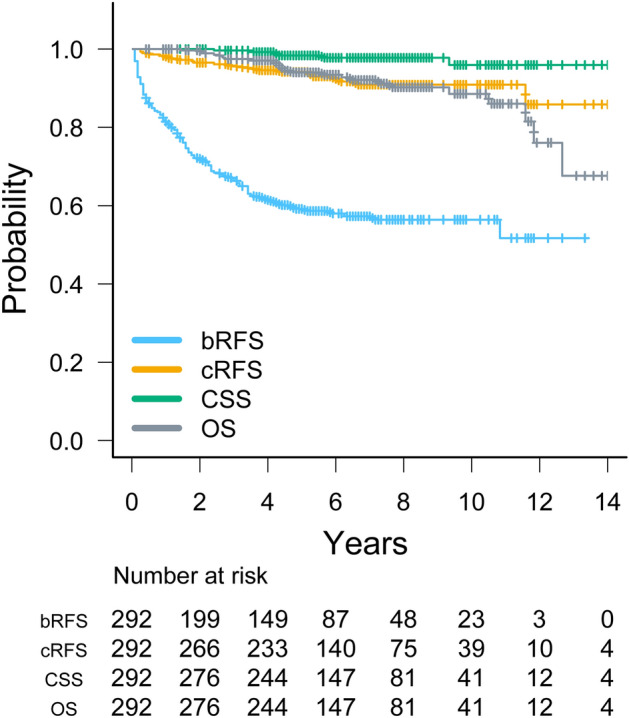
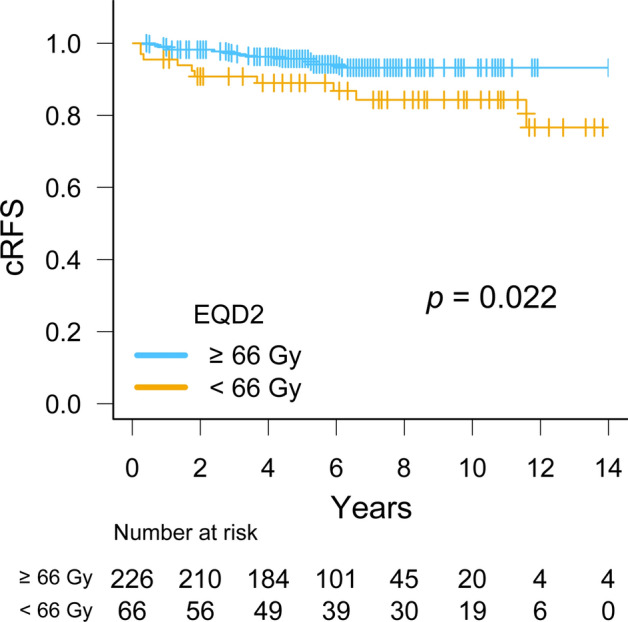
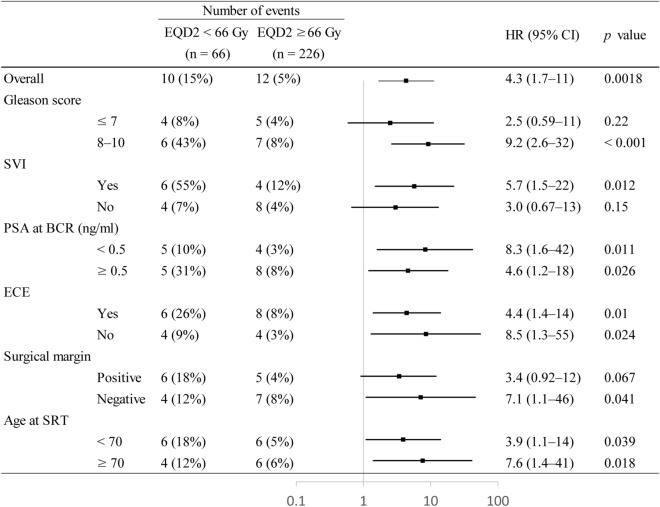
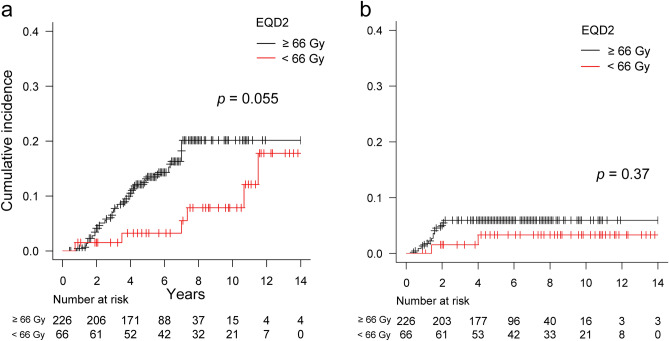
The relationship between radiation doses and clinical relapse in patients receiving salvage radiotherapy (SRT) for biochemical recurrence (BCR) after radical prostatectomy (RP) remains unclear. We identified 292 eligible patients treated with SRT between 2005 and 2018 at 15 institutions. Clinical relapse-free survival (cRFS) between the ≥ 66 Gy (n = 226) and < 66 Gy groups (n = 66) were compared using the Log-rank test, followed by univariate and multivariate analyses and a subgroup analysis. After a median follow-up of 73 months, 6-year biochemical relapse-free survival, cRFS, cancer-specific survival, and overall survival rates were 58, 92, 98, and 94%, respectively. Six-year cRFS rates in the ≥ 66 Gy and < 66 Gy groups were 94 and 87%, respectively (p = 0.022). The multivariate analysis revealed that Gleason score ≥ 8, seminal vesicle involvement, PSA at BCR after RP ≥ 0.5 ng/ml, and a dose < 66 Gy correlated with clinical relapse (p = 0.015, 0.012, 0.024, and 0.0018, respectively). The subgroup analysis showed the consistent benefit of a dose ≥ 66 Gy in patients across most subgroups. Doses ≥ 66 Gy were found to significantly, albeit borderline, increase the risk of late grade ≥ 2 GU toxicity compared to doses < 66 Gy (14% vs. 3.2%, p = 0.055). This large multi-institutional retrospective study demonstrated that a higher SRT dose (≥ 66 Gy) resulted in superior cRFS.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
High-dose salvage intensity-modulated radiotherapy with or without androgen deprivation after radical prostatectomy for rising or persisting prostate-specific antigen: 5-year results.Eur Urol. 2011 Oct;60(4):842-9. doi: 10.1016/j.eururo.2011.04.021. Epub 2011 Apr 16. Eur Urol. 2011. PMID: 21514039
-
Importance of the site of positive surgical margin in salvage external beam radiation therapy for biochemical recurrence of prostate cancer after radical prostatectomy.Cancer Med. 2018 May;7(5):1723-1730. doi: 10.1002/cam4.1408. Epub 2018 Mar 23. Cancer Med. 2018. PMID: 29573193 Free PMC article.
-
Dose-escalated salvage radiotherapy after radical prostatectomy in high risk prostate cancer patients without hormone therapy: outcome, prognostic factors and late toxicity.Radiat Oncol. 2013 Nov 27;8:276. doi: 10.1186/1748-717X-8-276. Radiat Oncol. 2013. PMID: 24279376 Free PMC article.
-
Salvage radiotherapy in prostate cancer patients with biochemical relapse after radical prostatectomy : Prolongation of prostate-specific antigen doubling time in patients with subsequent biochemical progression.Strahlenther Onkol. 2018 Apr;194(4):325-332. doi: 10.1007/s00066-017-1247-1. Epub 2017 Dec 18. Strahlenther Onkol. 2018. PMID: 29255924 English.
-
Improved biochemical outcome with adjuvant radiotherapy after radical prostatectomy for prostate cancer with poor pathologic features.Int J Radiat Oncol Biol Phys. 2005 Mar 1;61(3):714-24. doi: 10.1016/j.ijrobp.2004.06.018. Int J Radiat Oncol Biol Phys. 2005. PMID: 15708249
Cited by
-
A randomized study of apalutamide in Chinese patients with non-metastatic castration-resistant prostate cancer.iScience. 2025 Jul 18;28(8):113166. doi: 10.1016/j.isci.2025.113166. eCollection 2025 Aug 15. iScience. 2025. PMID: 40822333 Free PMC article.
References
-
- Ohri N, Dicker AP, Trabulsi EJ, Showalter TN. Can early implementation of salvage radiotherapy for prostate cancer improve the therapeutic ratio? A systematic review and regression meta-analysis with radiobiological modelling. Eur. J. Cancer. 2012;48:837–844. doi: 10.1016/j.ejca.2011.08.013. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
