

Surgical aortic valve replacement etiologies, hemodynamics, and outcomes in 1346 patients from the Malaysian heart centre
- PMID: 38167451
- PMCID: PMC10762830
- DOI: 10.1186/s13019-023-02472-2
Surgical aortic valve replacement etiologies, hemodynamics, and outcomes in 1346 patients from the Malaysian heart centre
Abstract
Background: This study examined the characteristics and outcomes of surgical aortic valve replacement (SAVR) both isolated and in combination with other cardiac surgery in Malaysia from 2015 to 2021.
Methods: This was a retrospective study of 1346 patients analyzed on the basis of medical records, echocardiograms and surgical reports. The overall sample was both considered as a whole and divided into aortic stenosis (AS)/aortic regurgitation (AR)-predominant and similar-severity subgroups.
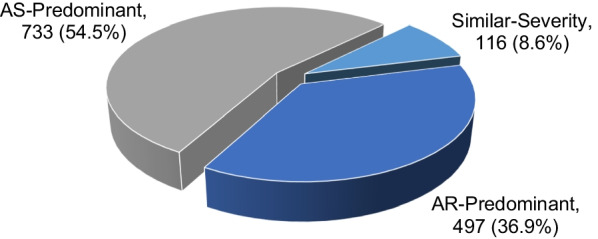
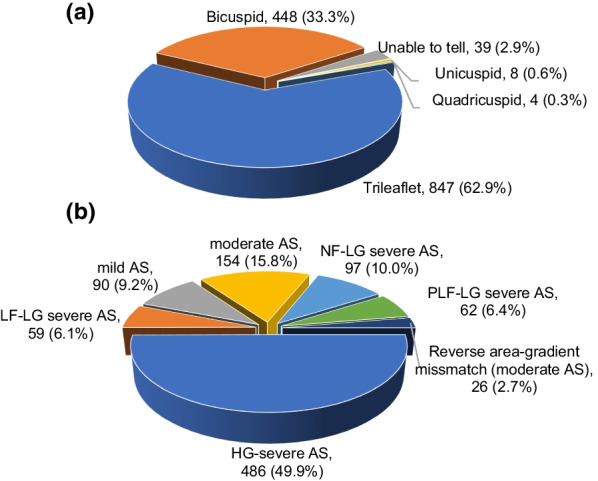
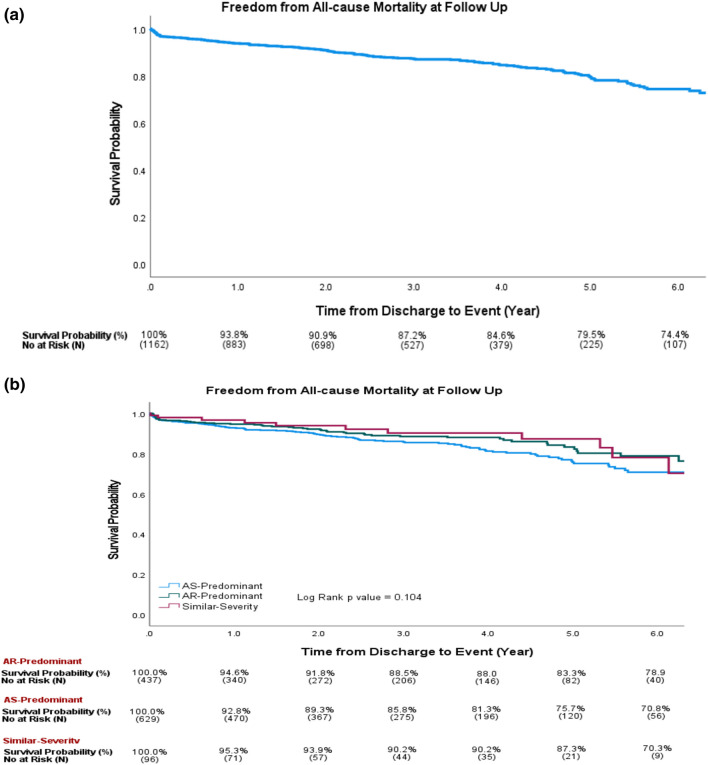
Results: The most common diagnosis was severe AS (34.6%), with the 3 most common etiologies being bicuspid valve degeneration (45.3%), trileaflet valve degeneration (36.3%) and rheumatic valve disease (12.2%). The second most common diagnosis was severe AR (25.5%), with the most common etiologies being root dilatation (21.0%), infective endocarditis (IE) (16.6%) and fused prolapse (12.2%). Rheumatic valve disease was the most common mixed disease. A total of 54.5% had AS-predominant pathology (3 most common etiologies: bicuspid valve degeneration valve, degenerative trileaflet valve and rheumatic valve disease), 36.9% had AR-predominant pathology (top etiologies: root dilatation, rheumatic valve disease and IE), and 8.6% had similar severity of AS and AR. Overall, 62.9% of patients had trileaflet valve morphology, 33.3% bicuspid, 0.6% unicuspid and 0.3% quadricuspid. For AS, the majority were high-gradient severe AS (49.9%), followed by normal-flow low-gradient (LG) severe AS (10.0%), paradoxical low-flow (LF)-LG severe AS (6.4%) and classical LF-LG severe AS (6.1%). The overall in-hospital and total 1-year mortality rates were 6.4% and 14.8%, respectively. Pure severe AS had the highest mortality. For AS-predominant pathology, the etiology with the highest mortality was trileaflet valve degeneration; for AR-predominant pathology, it was dissection. The overall survival probability at 5 years was 79.5% in all patients, 75.7% in the AS-predominant subgroup, 83.3% in the AR-predominant subgroup, and 87.3% in the similar-severity subgroup.
Conclusions: The 3 most common causes of AS- predominant patients undergoing SAVR is bicuspid valve degeneration, degenerative trileaflet valve and rheumatic and for AR-predominant is root dilatation, rheumatic and IE. Rheumatic valve disease is an important etiology in our SAVR patients especially in mixed aortic valve disease. Study registration IJNREC/562/2022.
Keywords: Aortic valve; Echocardiography; Etiology; Low gradient; Prosthesis.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interest.
Figures

References
-
- Liang-Choo H, Rajaram N. A review of acute rheumatic fever and rheumatic heart disease research in Malaysia. Med J Malaysia. 2016;71:79–86. - PubMed
-
- Durán AC, Daliento L, Frescura C, Stellin G, Sans-Coma V, Angelini A, et al. Unicommissural aortic valve in neonates and its association with other congenital heart disease. Cardiol Young. 1995;5(2):132–139. doi: 10.1017/S1047951100011707. - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
