

Persistent median artery and communicating branch related to the superficial palmar arch
- PMID: 38167619
- PMCID: PMC10762056
- DOI: 10.1038/s41598-023-50935-2
Persistent median artery and communicating branch related to the superficial palmar arch
Abstract
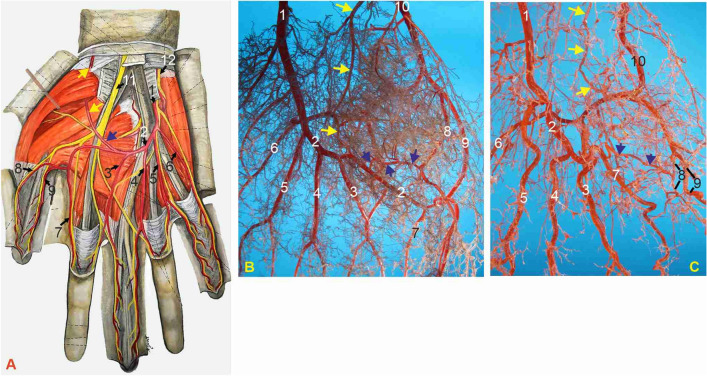
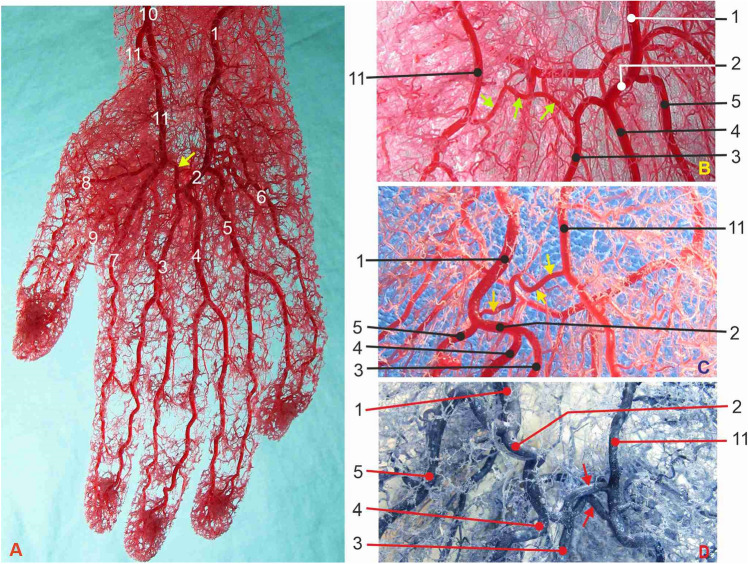
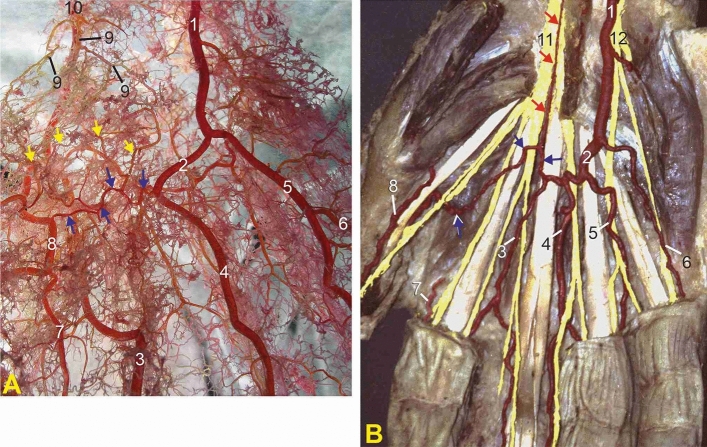
Microvascular surgery, plastic and reconstructive hand surgery, and coronary artery bypass surgery call for a microanatomical study of the branching pattern of the superficial palmar arch (SPA). For the anatomical analysis, we used a group of 20 dissected human hands injected with 4% formaldehyde solution and a 10% mixture of melted gelatin and India ink. The morphometric study was performed on 40 human hands of adult persons injected with methyl-methacrylate fluid into the ulnar and radial arteries simultaneously and afterwards corroded in 40% KOH solution for the preparation of corrosion cast specimens. The mean diameter of the SPA, between the second and third common palmar digital arteries, was 1.86 ± 0.08 mm. We identified the persistent median artery (PMA) in 5% of hands. We distinguished the three main groups of the SPAs according to variations in morphology and branching of the arch: Type 1, the long SPA; Type 2, the middle length SPA; and Type 3, the short SPA found in 27.5% of specimens. The communicating branch (CB), a vessel interconnecting the SPA to the closest branch of the radial artery, is classified into two different morphological groups. The third type of incomplete short arterial arch is the most important of the three groups of SPAs. That short SPA is potentially inadequate for restoring circulation after occlusion or radial artery harvesting for coronary artery bypass.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Waschke J, Bockers T, Paulsen F, editors. Sobotta Anatomy Textbook. Elsevier; 2019. pp. 188–189.
-
- Ross AC. Pectoral girdle and upper limb. In: Standring S, editor. Gray’s Anatomy. The Anatomical Basis of Clinical Practice. 42. Elsevier; 2021. pp. 980–982.
-
- Moore KL, Dalley AF, Agur AMR. Clinically Oriented Anatomy. Lippincott Williams and Wilkins; 2014. pp. 781–782.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
