

Microbial co-occurrences on catheters from long-term catheterized patients
- PMID: 38168042
- PMCID: PMC10762172
- DOI: 10.1038/s41467-023-44095-0
Microbial co-occurrences on catheters from long-term catheterized patients
Abstract
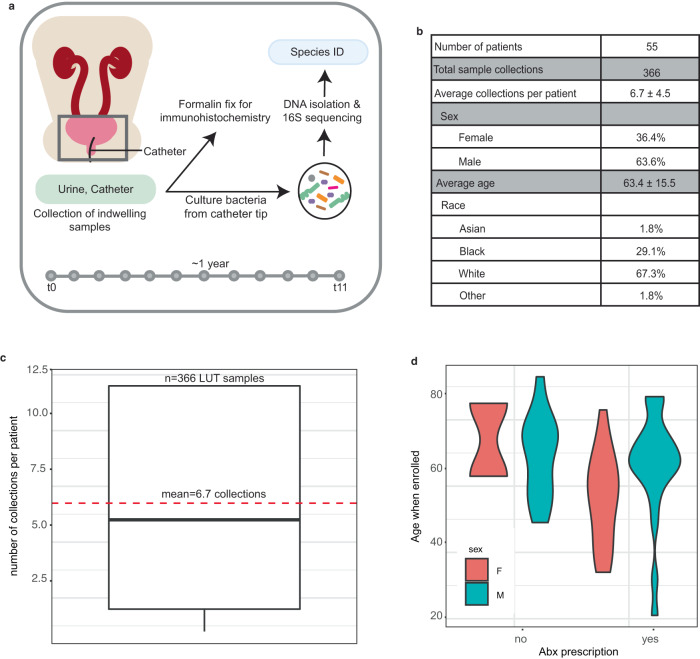
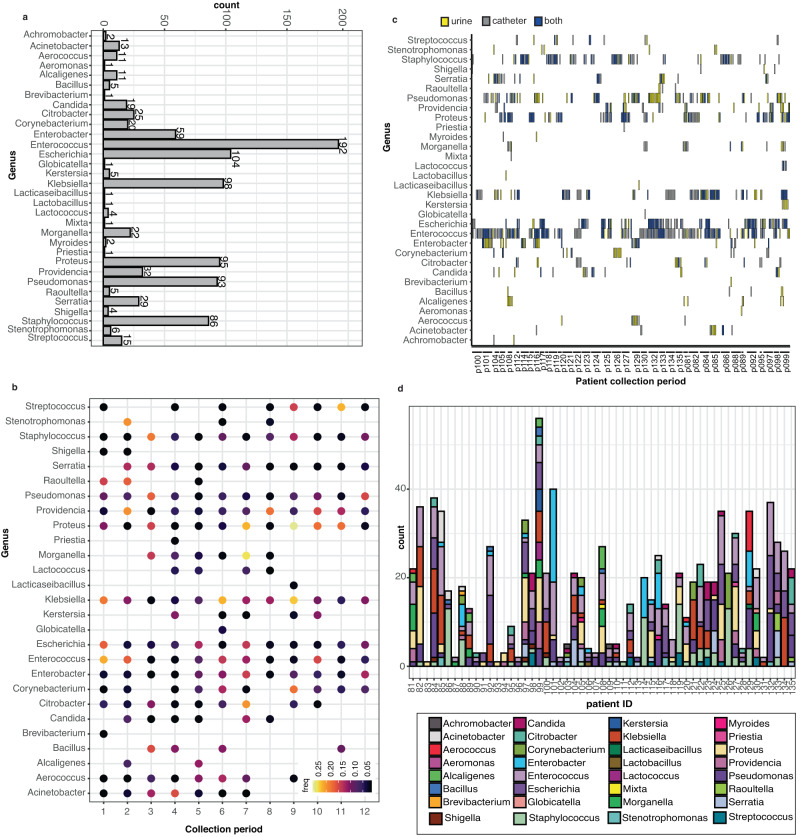
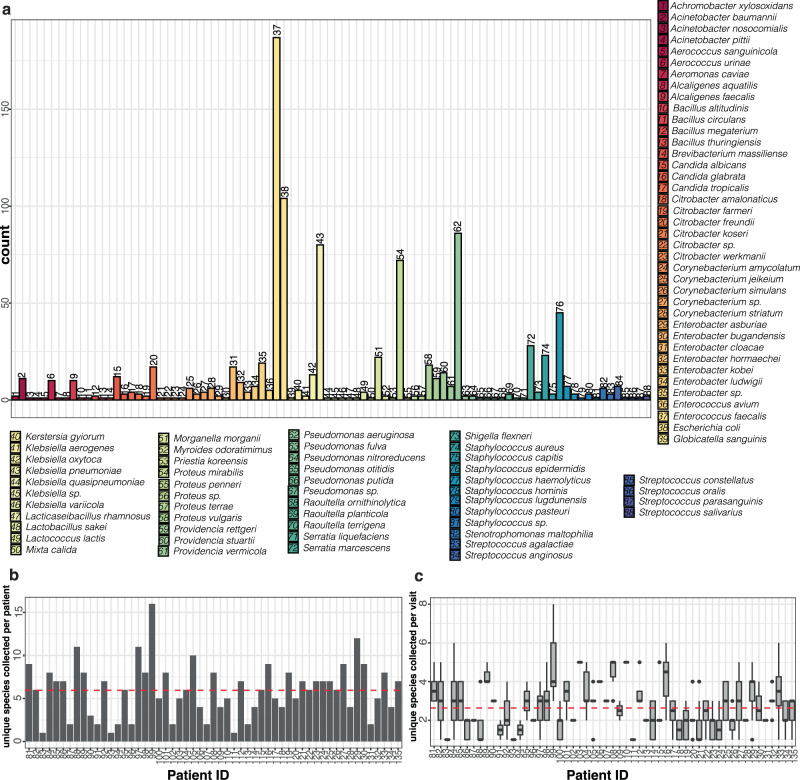
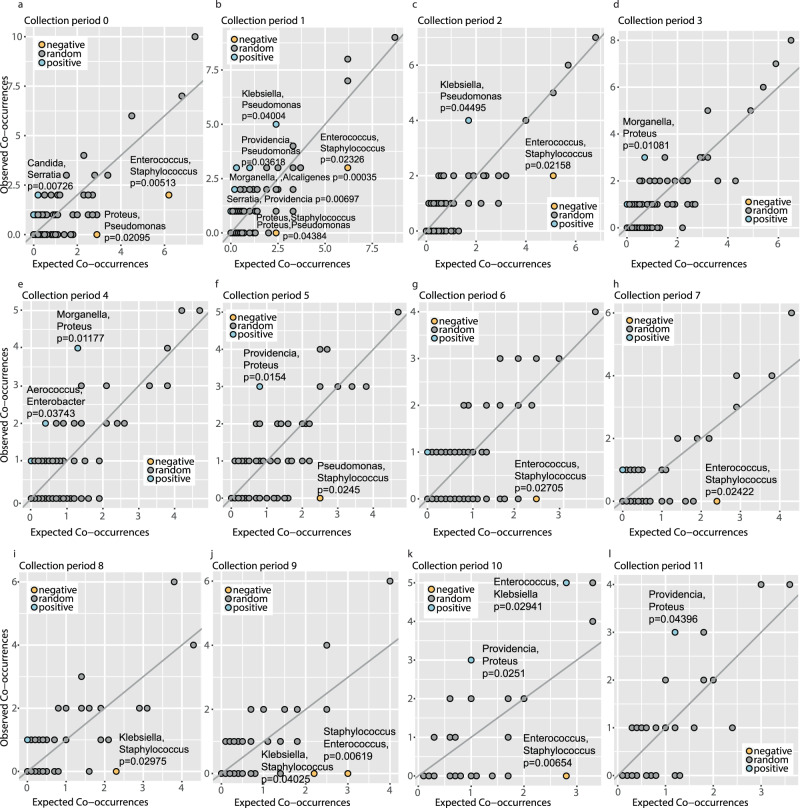
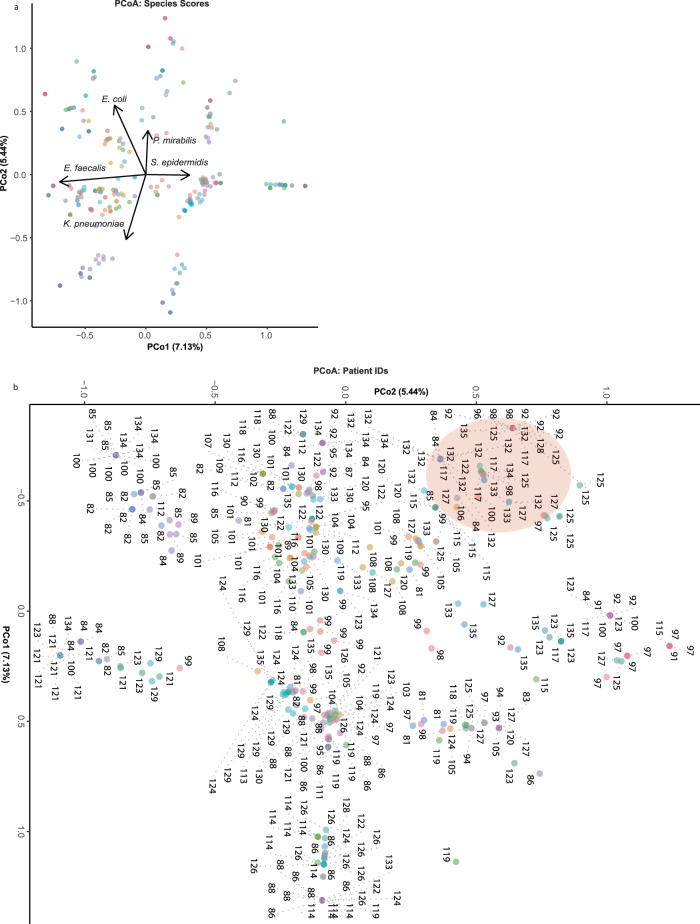
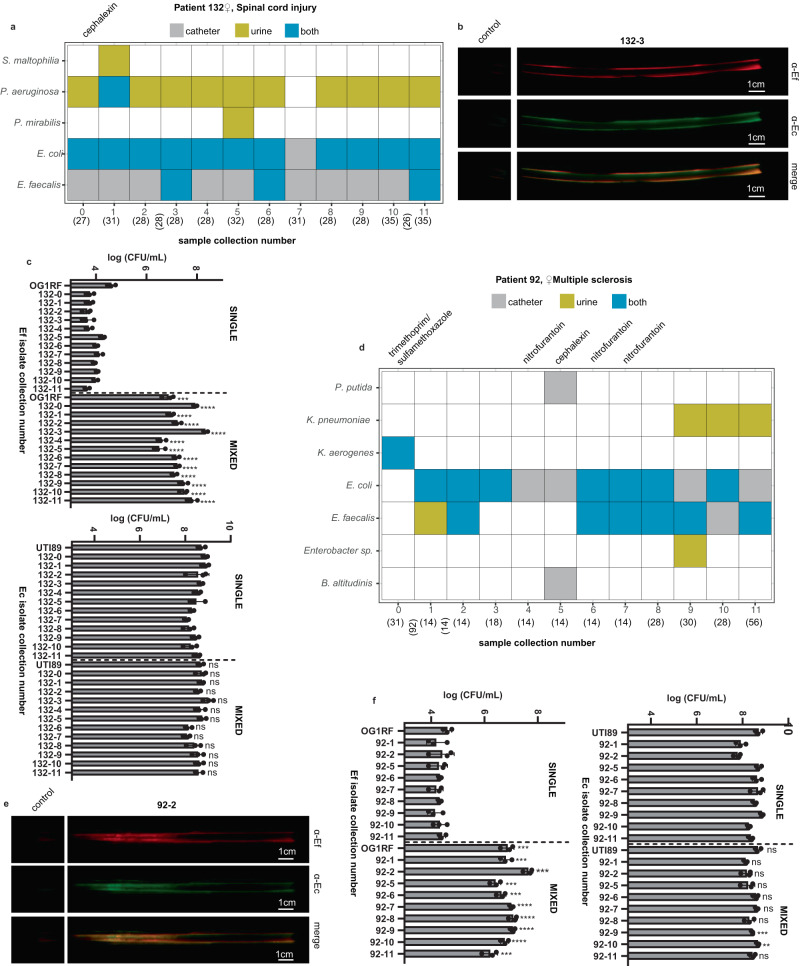
Catheter-associated urinary tract infections (CAUTIs), a common cause of healthcare-associated infections, are caused by a diverse array of pathogens that are increasingly becoming antibiotic resistant. We analyze the microbial occurrences in catheter and urine samples from 55 human long-term catheterized patients collected over one year. Although most of these patients were prescribed antibiotics over several collection periods, their catheter samples remain colonized by one or more bacterial species. Examination of a total of 366 catheter and urine samples identify 13 positive and 13 negative genus co-occurrences over 12 collection periods, representing associations that occur more or less frequently than expected by chance. We find that for many patients, the microbial species composition between collection periods is similar. In a subset of patients, we find that the most frequently sampled bacteria, Escherichia coli and Enterococcus faecalis, co-localize on catheter samples. Further, co-culture of paired isolates recovered from the same patients reveals that E. coli significantly augments E. faecalis growth in an artificial urine medium, where E. faecalis monoculture grows poorly. These findings suggest novel strategies to collapse polymicrobial CAUTI in long-term catheterized patients by targeting mechanisms that promote positive co-associations.
© 2024. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Scott, R. D. The Direct medical costs of healthcare-associated infections in U.S. hospitals and the benefits of prevention. In Division of Healthcare Quality Promotion, National Center for Preparedness, Detection, and Control of Infectious Diseases, Centers for Disease Control and Prevention (eds Polock, D. A. & Stone, P. W.) (2009). https://www.cdc.gov/hai/pdfs/hai/scott_costpaper.pdf.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
