

Cytokine signature in convalescent SARS-CoV-2 patients with inflammatory bowel disease receiving vedolizumab
- PMID: 38168138
- PMCID: PMC10761911
- DOI: 10.1038/s41598-023-50035-1
Cytokine signature in convalescent SARS-CoV-2 patients with inflammatory bowel disease receiving vedolizumab
Abstract
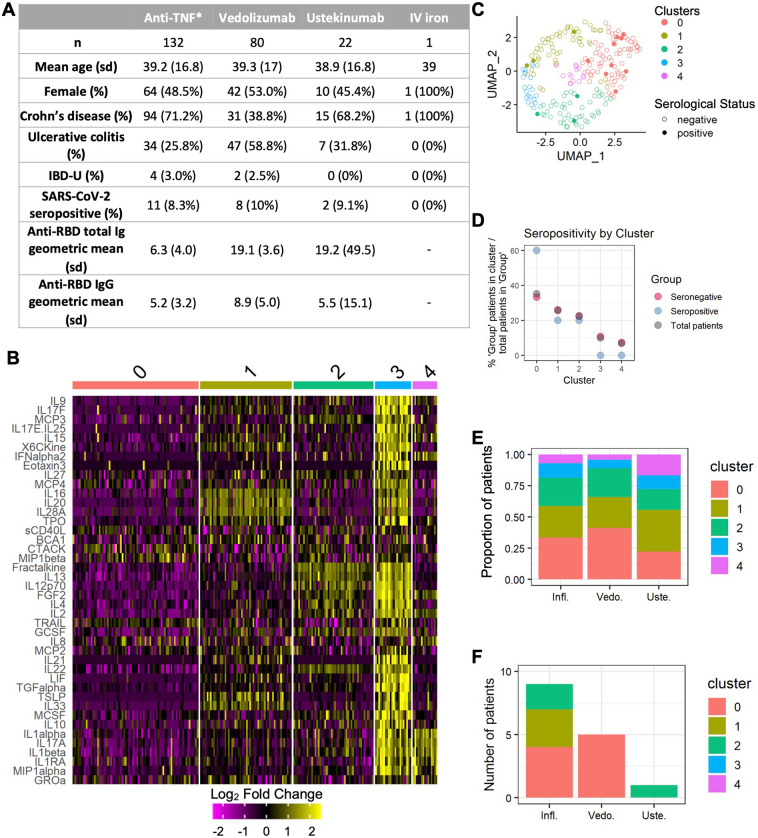
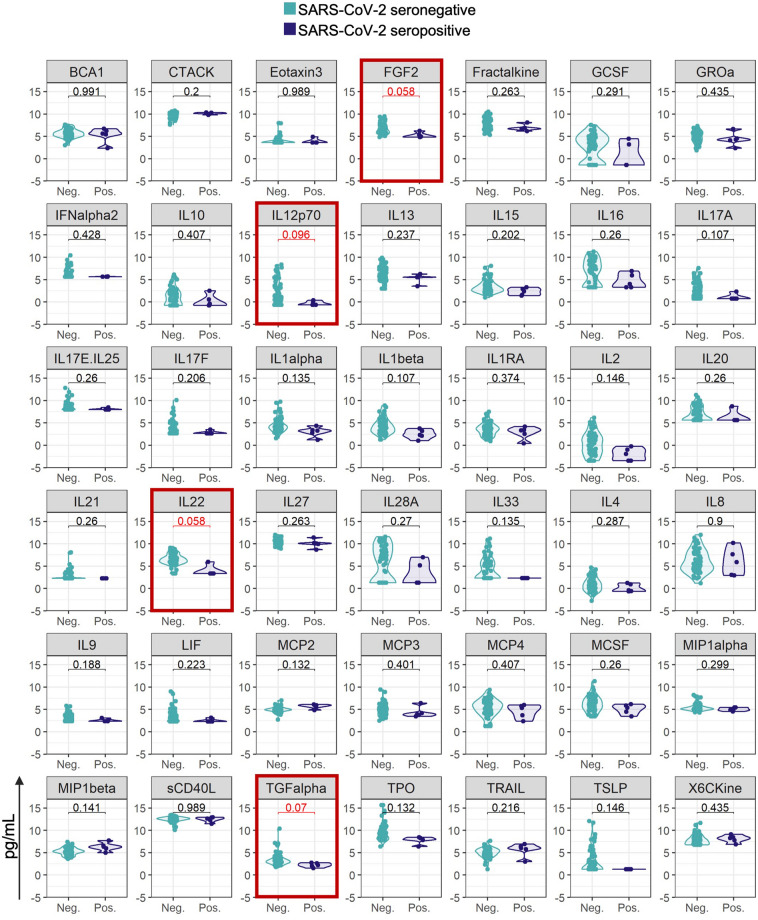
While differential antibody responses SARS-CoV-2 in patients with inflammatory bowel disease (IBD) receiving infliximab and vedolizumab are well-characterized, the immune pathways underlying these differences remain unknown. Prior to COVID-19 vaccine development, we screened 235 patients with IBD receiving biological therapy for antibodies to SARS-CoV-2 and measured serum cytokines. In seropositive patients, we prospectively collected clinical data. We found a cytokine signature in patients receiving vedolizumab who are seropositive compared with seronegative for SARS-CoV-2 antibodies that may be linked to repeated SARS-CoV-2 infections. However, there were no differences between seropositive and seronegative patients receiving infliximab. In this single-center cohort of patients with IBD with anti-SARS-CoV-2 antibodies at the onset of the COVID-19 pandemic, and therefore without influence of vaccination, there is a cytokine signature in patients receiving vedolizumab but not infliximab. These findings lay the groundwork for further studies on immune consequences of viral infection in patients with IBD, which is postulated to evolve from aberrant host-microbe responses.
© 2024. The Author(s).
Conflict of interest statement
SD, VMP, JME, JW, CT have nothing to disclose. SYW receives grants from the NCI SeroNet, the Crohn’s and Colitis Foundation, New York Crohn’s and Colitis Foundation, and TriNetX; and has received speaker fees from Crohn’s and Colitis Congress and Physicians’ Education Resource. JS has grant funding from UKRI, ECCO, and European Commission, and serves as Director of the UK IBD Registry; and is a member of the Independent Advisory Group to UK Government on management of COVID-19 in vulnerable individuals. JFC receives grants from AbbVie, Janssen Pharmaceuticals and Takeda; serves as consultant for AbbVie, Amgen, Arena Pharmaceuticals, Boehringer Ingelheim, BMS, Celgene Corporation, Eli Lilly, Ferring Pharmaceuticals, Galmed Research, Genentech, Galxo Smith Kline, Janssen Pharmaceuticals, Kaleido Biosciences, Imedex, Immunic, Iterative Scopes, Merck, Microba, Novartis, Otsuka Pharmaceutical Development PBM Capital, Pfizer, Protagonist Therapeutics Sanofi,Takeda, TiGenix, Vifor; received speaker fees from AbbVie, Amgen, Allergan, Inc. Ferring Pharmaceuticals, Shire, and Takeda; and holds stock from Intestinal Biotech Development. KC receives funding from US National Institute of Health (NIH) grants HL123340, DK093668, AI140754, AI121244, AI130945, DK124336, the Kenneth Rainin Foundation, Pfizer, and Takeda-Columbia-NYU Alliance; has severed as consultant for or received speaker fees from Puretech Health, Abbvie, and Genentech.
Figures
References
-
- Kennedy NA, Goodhand JR, Bewshea C, et al. Anti-SARS-CoV-2 antibody responses are attenuated in patients with IBD treated with infliximab. Gut2021. p. gutjnl-2021–324388. - PubMed
-
- Lin S, Kennedy NA, Saifuddin A, et al. Antibody decay, T cell immunity and breakthrough infections following two SARS-CoV-2 vaccine doses in inflammatory bowel disease patients treated with infliximab and vedolizumab. Nat. Commun. 2022;13(1):1379. doi: 10.1038/s41467-022-28517-z. - DOI - PMC - PubMed
-
- Wellens J, Edmans M, Obolski U, et al. Combination therapy of infliximab and thiopurines, but not monotherapy with infliximab or vedolizumab, is associated with attenuated IgA and neutralisation responses to SARS-CoV-2 in inflammatory bowel disease. Gut. 2021 doi: 10.1136/gutjnl-2021-326312. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
